
Rajeev P. Nagassar, Roma J. Bridgelal-Nagassar, Keston Daniel, Lima Harper
Correspondence:
Dr Rajeev P. Nagassar
Department of Microbiology
Sangre Grande Hospital
Ojoe Road
Sangre Grande
Email: [email protected]
Copyright: This is an open-access article under the terms of the Creative Commons Attribution License which permits use, distribution, and reproduction in any medium, provided the original work is properly cited.
©2021 The Authors. Caribbean Medical Journal published by Trinidad & Tobago Medical Association
ABSTRACT
Objectives
To assess the compliance of hand hygiene (HH) practices of staff and determine the impact of multimodal interventions to improve hand hygiene practices.
Methods
A prospective study was conducted to determine the hand hygiene (HH) practices of staff according to the World Health Organization’s “5 moments of HH”. During random visits to the general wards, HH practices of staff were observed for 41 weeks during 2014-15. During the first 8 weeks, the basic compliance rate (BCR) was calculated. A BCR of 50% or more was considered compliant. Data were provided to the staff via email. Toolbox talks, posters, and other educational interventions were instituted in a multimodal manner. Wards were visited by infection control staff to reinforce HH practices. During the post-intervention phase, the HH practices were reassessed for 33 weeks to compare the impact of interventions.
Results
A total of 13,120 observations were made. Participants ranged from ages 18 to 65. The overall average BCR before intervention was 34.1%, for the first 8 weeks, while it increased to 62.3%, over the next 33 weeks, after the multimodal interventions (p =0.007). The wards which showed significant improvement include Paediatrics (p <0.0001), Male Surgical (p = 0.001), Female Surgical (p = 0.005), Male Medical (p < 0.0001), Haemodialysis Unit (p < 0.0001), ICU, (p = 0.038), and Accident and Emergency (p = 0.007). Obstetric, Female Medical, and Oncology wards did not show statistically significant improvement.
Conclusion
Hand Hygiene compliance rate of staff can be improved by multimodal interventions in a General Hospital setting.
Introduction
Proper hand hygiene (HH) is essential for adequate infection control. This is because transmission of pathogens occurs primarily by hands [1]. Compliance rates of hand hygiene practices among health care workers have been shown to be unacceptable, with less than 50% compliance being reported in many institutions in the United States [1].
A barrier to good HH is lack of knowledge among personnel. Additionally, lack of understanding of correct HH techniques, understaffing and overcrowding and poor access to hand washing facilities are also barriers. Irritant, contact dermatitis associated with frequent exposure to soap and water and lack of institutional commitment to good HH are additional factors [2, 3]. The World Health Organization (WHO) has recognized the importance of good HH [2, 4].
‘Five moments of HH’, according to WHO, includes any actions, ‘before’, ‘during’ touching a patient (before aseptic technique, after blood and body fluids and patient contact) and ‘after contact with the patient surroundings’ [4]. These moments form the core opportunities healthcare workers should comply with and wash or rub their hands with antiseptics. WHO recommends auditing every hospital in accordance with these five moments [4, 5].
In an article by Pittet et al, it was shown that HH rates varied by hospital wards [6]. On the same token it has also been well established that as HH compliance improved, the incidence of nosocomial infections decreased [2, 7].
With this background, this study was designed to test the basic compliance rate among staff according to the ‘five moments of HH’ using the WHO BCR audit and calculation tool and also test the impact of multimodal interventions to improve the hand hygiene practices of the staff in a District General Hospital in Trinidad.
Methods
After institutional approval by the Eastern Regional Health Authority Ethics Committee, a cross-sectional study was undertaken for a total of 41 weeks during the period from October 2014 to August 2015. This included 8 weeks of observation before interventions to determine the basic compliance rate of staff for HH practices, followed by interventions and simultaneous measurements of practices in the post-intervention phase for 33 weeks. Staffs were assigned specifically for auditing HH, according to WHO standards. A lottery method was used to randomize different auditors to different wards at different times. Auditors thus visited wards at different times and on different days every week. Auditing targeted all categories of staff on the ward at that time. Observation of the same staff member on different days was considered different observations.
Compliance was assessed covertly by direct observation weekly at the individual level by a trained HH auditor using the paper version of the WHO-BCR HH audit sheet. The audit sheet for specific HH moments were not used in this study. All observations were collected between 7:30 am and 3:30 pm. Each observation session lasted 2 hours, during which time at least three different members of staff were followed covertly, in their duties.
Where possible, every effort was made to conceal who were auditing the staff and thus reduce the Hawthorne effect. This study encompassed all wards at the SGH. HH compliance was expressed as the ratio of the number of performed actions to the number of opportunities. This was calculated as follows:
Basic compliance rate (BCR) (%) = performed actions/ opportunities ˣ 100.
A BCR of 50% or more was considered compliant, while less than 50% was considered non-compliant. Sample size was calculated, using Raosoft® calculator. 377 observations were needed, divided among the various wards and staff categories.
Pre and Post-Intervention
This study had a pre-intervention period of 8 weeks of monitoring BCR. This was followed by a planned stepwise multimodal behavioral improvement approach. It focused on education and feedback of the results of auditing BCR rates from week 9 onwards. Feedback was by tool box talks, emails and using posters displaying the 5 moments of HH, where necessary. At the start of the intervention tool box talks were given to each ward/unit, in which the health care worker was be informed about the 5 moments of HH and proper hand washing techniques. Eight (8) weeks after the start of BCR monitoring, the intervention measurements commenced and hence 33 weeks of post-intervention monitoring of BCR was done.
The key elements of the intervention were as follows: Data of the audit was provided to the staff via email. Reports were compiled weekly and sent to all staff at the end of the week. If non-compliance was observed, the ward was also visited by infection control staff to reinforce HH practices and investigate causes of non-compliance. In addition, tool-box talks and posters were put up to reinforce HH educational activities. The ward staff received one to two tool-box group sessions during the period of 33 weeks. The tool-box talks were led by two specially trained HH auditors and the infection control nurse. During the intervention period, the infection control nurse and HH auditors actively supported the staff in HH compliance on the wards. In order to increase the chances of successful implementation, an extensive communication strategy was put in place prior to the start of the intervention period. Trained auditors and the infection prevention and control nurse were appointed under the guidance of the medical microbiologist; they acted as coordinators for all multimodal activities and educated staff post-intervention.
Statistical analyses were undertaken to see if there was a difference between the BCRs in the pre-intervention and post-intervention periods. Inferential tests included Chi-square test and t-tests as appropriate. A p value of < 0.05 was considered statistically significant. The software Statistical Package for Social Sciences (SPSS) – version 20 (IBM, USA) was used for statistical analyses.
Results
During the eleven months of study, a total of 13,120 observations were recorded. Participants belonged to both genders and ranged from ages 18 to 65 years. A total of ten locations covering the whole hospital were included in the study, which included adult medical and surgical wards, pediatric and oncology wards, haemodialysis unit, intensive care unit (ICU) and Accident & Emergency (A&E).The distribution of HH observations according to department is shown in Figure 1. Over 1000 observations were made per ward, as illustrated.

When all wards were considered, the overall average BCR before intervention was 34.1%, for the first 8 weeks, while it increased to 62.3%, for the next 33 weeks, after the multimodal interventions were implemented. This improvement was statistically significant (p =0.007). The individual BCRs in each ward before and after interventions and the comparison are detailed in Table 1.

The following wards showed significant improvement in their staff HH practices after multimodal interventions: Ward 1 (Pediatrics),p <0.0001, Ward 2 (Male Surgical) p = 0.001, Ward 3 (Female Surgical) p = 0.005, Ward 6 (Male Medical), p < 0.0001, Haemodialysis Unit, p < 0.0001, ICU, p = 0.038, and Accident and Emergency, p = 0.007. Wards which did not show statistically significant improvement included: Ward 4 (Obstetrics), p = 0.058, Ward 5 (Female Medical), p = 0.13, and Oncology ward, p = 0.078.
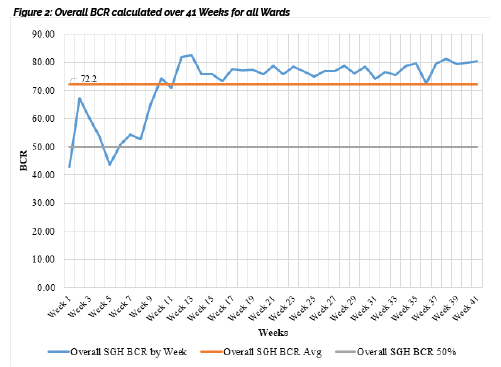
The run chart in Figures 2 shows the average BCR for the SGH over the 41 week period of this study. It clearly illustrates a significant increase in compliance between Week 8 -14. The BCR steadily rose from 52.81 to 75.66, with commencement and the continuation of the education and promotion activities (multimodal intervention). Throughout the remaining study period it showed maintenance of a steady compliance rate from week 14 onwards.
Discussion
This study found that hand hygiene BCR rates can be significantly improved in the staff of a General Hospital by proactive, multimodal interventions. The strengths of the study include a reasonably large sample size on all wards, which might have contributed to the robustness and power of this study. Ina general hospital setting, it is important that all wards have good HH practices and a high BCR of these practices for reduction of transmission of infection [7, 8]. Multimodal interventions such as prospective audit and feedback with use of tool-box talks and poster reminders were an integral part of maintaining sustained HH compliance post-intervention on most wards. The findings of the study clearly establish this overall improvement in the whole hospitals as well as majority of the wards and furthermore there was sustained improvement in HH practices throughout the 33 weeks of post-intervention phase, as shown by the run charts.
Published literature have conflicting results on the benefits of interventions as it relates to HH practices. Huang et al and Gould et al studied the effect of educational impact, such as feedback and enforcement of HH procedures, and concluded that the effect remains unclear. Huang et al showed significant increase in compliance, four months after intervention, but Gould et al showed no improvement at all after intervention [9, 10]. In the present study, not only there was significant improvement in the BCR, but also the overall HH compliance remained significantly sustained over the 33-weeks post-intervention, following multimodal intervention, similar to the report by Huang et al. Some wards which showed no significant change with the multimodal intervention, when looked at individually, may be comparable to the report by Gould et al.
Additionally, basic observation of the HH practices and providing immediate feedback to the staff has been shown to be a moderately effective method of increasing HH compliance as shown by Fuller HH et al [11]. In this stepped wedge cluster randomized controlled trial, they showed that combining feedback to intervention produced moderate but significant sustained improvements in HH compliance in wards. This is similar to the overall sustained increased compliance rate seen in the present study.
There could have been many reasons for the sustained improvement of the HH practices of the staff in the various locations of the hospital. The infection control staff were very proactive, conducting intermittent audit and providing feedback of HH BCR. Thus, a sustained compliance effect on HH BCR was accomplished post-intervention, on most wards. This may also have occurred through behavioral modifications in the multimodal interventions. Stewardson et al showed sustained compliance, as in the present study, but there was no clinical significance of their multimodal intervention compared to control [12]. In this randomized control trial of multimodal behavioral intervention to improve hand hygiene by Stewardson et al, the difficulty of behavioral change was noted. Our study did not specifically look into the behavioral modifications of the staff, although the multimodal interventions did target the behavioral changes paradigm.
It should be noted that although oncology, obstetrics and female medical wards showed no statistically significant improvement in BCR before and after intervention, the baseline BCRs themselves were higher than the set threshold value for compliant BCR, which is 50%. These three wards were seen to have similar pre-intervention and post-intervention BCRs and thus there was no significant change in BCR observed with the multimodal intervention, on these wards. A short pre-intervention compared to post-intervention, the Hawthorne effect and observer biases are some of the factors that could have accounted for this also. Thus all wards in the hospital displayed BCRs in the compliant range, however oncology, obstetrics and female medical showed no significant change with the instituted multimodal intervention, in this study. Thus factors other than the multimodal intervention, in this study, may have contributed to the small rise in BCRs seen in these wards [9-12].
It is possible that in this current study at the Sangre Grande Hospital, there may have been difficulties with behavior change, accounting for the insignificant findings seen in oncology, obstetrics and female medical wards [12-14]. The main limitation of this study was that it did not assess the effect of HH on nosocomial infection rates [6, 14]. Thus, further study may be needed to correlate the nosocomial infection rates of individual wards with HH practices as well as to elucidate the reasons for the small and insignificant increase in BCRs seen in oncology, obstetrics and female medical wards.
CONCLUSION
Multimodal interventions, with a target of behavior modification, appeared successful in this study, overall.
References
1. Lankford MG, Zemblower TR, Trick WE, Hacek DM, Noskin GA, Peterson LR. Influence of role models and hospital design on hand hygiene of healthcare workers. Emerg Infect Dis. 2003; 9: 217-23.
2. Centres for Disease Control and Prevention (CDC), the Association for Professionals in Infection Control and Epidemiology (APIC), and the Society of Healthcare Epidemiology of America (SHEA). How-to Guide: Improving Hand Hygiene. A Guide for Improving Practices among Health Care Workers. Accessed (20th October 2016). Available from: http://www.sheaonline.org/Assets/files/IHI_Hand_Hygiene.pdf
3. Pittet D, Boyce JM. Hand hygiene and patient care: Pursuing the Semmelweis legacy. Lancet Infect Dis. 2001; 1: 9-20.
4. WHO Guidelines on Hand Hygiene in Health Care (Advanced Draft): A Summary. World Health Organization; 2005. Accessed (20th October 2016). Available from: http://www.who.int/patientsafety/events/05/HH_en.pdf
5. Boyce JM, Pittet D, et al. Guideline for Hand Hygiene in Health-Care Settings: Recommendations of the Healthcare Infection Control Practices Advisory Committee and the HICPAC/SHEA/APIC/IDSA Hand Hygiene Task Force. Morbid Mortal Wkly Rep. 2002; 51(RR16):1-45.
6. Pittet D. Improving Adherence to Hand Hygiene Practice: A Multidisciplinary Approach. Emerg Infect Dis. 2001; 7 (2): 234-40.
7. Pittet D, Hugonnet S, Harbarth S etal. Effectiveness of a hospital-wide program to improve compliance with hand hygiene. Lancet. 2000; 356:1307-12.
8. Pittet D, Dharank,l S, Touveneau S, Savan V, Perneger TV. Bacterial contamination of the hands of hospital staff during routine patient care. Arch Intern Med. 1999; 159: 821-6.
9. Gould D J, Chamberlain A. The use of a ward-based educational teaching package to enhance nurses’ compliance with infection control procedures. J Clin Nurs. 1997; 6(1):55–67.
10. Huang J, Jiang D, Wang X, Liu Y, Fennie K, Burgess J, et al. Changing knowledge, behavior and practice related to universal precautions among hospital nurses in China. J Contin Educ Nurs. 2002; 33(5): 217–24.
11. Fuller C, Michie S, Savage J, McAteer J, Besser S, Charlett A, et al. (2012) The Feedback Intervention Trial (FIT) — Improving Hand-Hygiene Compliance in UK Healthcare Workers: A Stepped Wedge Cluster Randomised Controlled Trial. PLoS ONE. 7(10): e41617. https://doi.org/10.1371/journal.pone.0041617.
12. Stewardson AJ, Sax H, Gayet-Ageron A. Enhanced performance feedback and patient participation to improve hand hygiene compliance of health-care workers in the setting of established multimodal promotion: a single-center, cluster randomized controlled trial. Lancet Infect Dis. 2016; 16 (12): 1345 – 1355.
13. Al-Hussami M, Darawad M, Almhairat I.I. Predictors of compliance hand washing practice among healthcare professionals. Healthcare Infection. 2011; 16: 79–84.
14. Gould DJ, Moralejo D, Drey N et al. Interventions to improve hand hygiene compliance in patient care. Cochrane Database Syst Rev. 2010; (9):CD005186. doi: 10.1002/14651858.CD005186.pub3.