

Correspondence to:
Professor S Hariharan
Professor of Anaesthesia & Critical Care Medicine
Anaesthesia & Intensive Care Unit
Faculty of Medical Sciences
The University of the West Indies, St. Augustine
Trinidad, Trinidad & Tobago
Tel/fax: 1 868 662 4030
Email: [email protected]
Abstract
Objectives
To determine the prevalence of pain among adult patients attending outpatient clinics in Trinidad and the factors associated with the higher prevalence of chronic pain.
Methods
A direct face-to face survey was conducted in adult patients of the medical and surgical outpatient clinics of the major hospitals. Data recorded included demographics, clinical information. A Numerical Pain Rating Scale (NRS) was used to quantify the intensity of pain. Patient perceptions regarding the chronic pain was captured by a 6-item questionnaire in a 5-point Likert Scale.
Results
A total of 621 adult patients were studied. Overall, acute pain was prevalent in 13% and chronic pain in 56% of the outpatients. Majority of the patients ranked their pain severity as 8 and 10 on the NRS. Pain was commonly affecting back and lower limbs. Older age, female gender, East Indian ethnicity and surgical conditions predisposed to higher prevalence of pain. Although 90% of the patients were treated with analgesics, 33% were dissatisfied with the management. More than 80% of patients felt that their chronic pain affected their quality of life and 64% felt it caused financial burden in their life.
Conclusion
The prevalence of pain is high in adult Trinidadian outpatients. Pain was of severe intensity, commonly affected the back and lower limbs. Many patients were not satisfied with their current treatment. There is a need for establishing pain clinics in the public healthcare system of Trinidad & Tobago.
Introduction
The International Association for the Study of Pain (IASP) defines pain to be a subjective phenomenon and a psychological state [1]. It is the most common symptom treated by any physician. When acute pain disorders such as postoperative pain and trauma pain have clear pathophysiological explanations of nociceptive processes, chronic pain has not been always that clearly definable in terms of nociception alone. Chronic pain is usually defined as persistent pain lasting for more than 12 weeks [2]. Most chronic pain syndromes are either neuropathic or non-neuropathic in origin and are influenced by multiple factors including age, gender, cultural background, occupation, psychosocial status, economic background etc., which may influence both the prevalence as well as the intensity of chronic pain.
Chronic pain, especially low back pain, has been recognized as one of the leading causes of ‘global burden’ of diseases listed by the World Health Organization. The overall prevalence of chronic pain in the general population globally is estimated to be around 20%, also attributable to 15-20% of visits to physicians [3-8]. The prevalence of chronic pain in Canada has been shown to be around 15%, while it is 19% in New Zealand [9, 10]. A recent study from Israel found a very high prevalence of around 55% of chronic pain syndromes in the elderly age group individuals (≥65 years) living in the community [11]. Even in Denmark, which is highly ranked according to the UN Human Development Index, the prevalence of chronic pelvic pain in females was reported to be in the range of 2 – 21% [12].
Although these reports comprise of the prevalence of pain in the general population, there have been many published studies from throughout the world, which report a wide range of prevalence of pain in patients within the hospital settings also [13-17].
Chronic postoperative pain is one of the less acknowledged yet most troublesome and important outcomes of surgery, with approximately 10-50% of surgical patients subsequently developing chronic pain conditions related to their procedure [18-20].
The above facts suggest that pain is highly prevalent both in the general population as well as hospital settings throughout the world. Hence there is a possibility that it may be of a major concern in Trinidad as well. However, to our knowledge, there has been no published literature regarding the prevalence of pain in the hospital settings of Trinidad & Tobago. There is a gap in public awareness regarding chronic pain, probably due to the absence of established pain clinics in the country. Hence this study attempted to strengthen the evidence regarding the prevalence of acute and chronic pain in patients attending the public hospitals of Trinidad & Tobago so that adequate measures are put in place to meet the needs of the common citizens seeking free healthcare.
With this background, the primary objective of the current study was to determine the prevalence of acute and chronic pain in a purposive-sample, selected-group of patients attending the outpatient clinics in the three major General Hospitals of Trinidad & Tobago. The secondary objectives of the study were to determine the socio-demographic and clinical factors which may be associated with the prevalence of pain. This may assist policy-makers to specifically target the factors attributable to the development of pain as well as persons who are much more susceptible to suffer from pain, and eventually assist them by commissioning pain clinics in the public healthcare system.
Methods
Approval was obtained from the University Ethics Committee of the Faculty of Medical Sciences, St. Augustine prior to the study, and a signed informed consent was required from every patient. Outpatient clinics from each of the three major teaching hospitals in Trinidad were selected. To allow a wider cross-section of patients, orthopaedic surgery, general surgery and urology clinics were selected in the surgical specialties, and cardiology, neurology, haematology, and general medicine clinics were selected within the medical specialties.
The purposive sampling method was adopted and the questionnaires were administered to adult patients exclusively. Exclusion criteria included pregnant women and mentally ill persons. Willing participants were asked to sign an informed consent after sufficient discussion. Explanations were given to the participants including details regarding confidentiality, their knowledge and comprehension of the research. This was done to enable them to make a comfortable decision about participating in the study.
Baseline data collected included demographics (age, sex, race, monthly income, and educational level), underlying systemic disorders, clinic attended, duration of pain, nature, and location of pain and current methods of treatment. For the purpose of this study, chronic pain was defined as pain persisting in a patient for a duration of more than three months. The instrument utilized for data collection on the impact of chronic pain was a 6-item questionnaire that was conceived de novo, developed to capture information from the patients suffering from chronic pain. The predominant information captured by this questionnaire was the individual patient’s perceptions of their pain and how it affects their livelihood. Investigators read each and every question to participants and recorded the responses in order to minimize collecting wrong information. Participants with chronic pain were also asked to rate the intensity of their pain using a Numerical Pain Rating Scale ranging between 1 – 10, with 1 being the mildest and 10 being the most severe intensity.
Descriptive analyses of the data were done to determine the central tendencies and the distribution of data. Inferential analyses included one-way analysis of variance (ANOVA) and Chi-square analysis to compare different groups. The statistical significance was fixed at the level of p<0.05. The statistical software – Statistical Package for Social Sciences (SPSS) – version 13 was used for analyses.
Results
A total of 621 respondents, who were patients attending the outpatient clinics in the three major hospitals were surveyed over a period of consecutive three months.
There was a comparable distribution of the respondents among the three hospitals; Hospital I comprised of 209 (34%) of the total, Hospital II: 200 (32%) and Hospital III: 212 (34%). Overall, 316 (51%) respondents belonged to the surgical outpatient clinics and 305 (49%) belonged to the medical outpatient clinics. The distribution of respondents within the specialties is shown in Table 1.
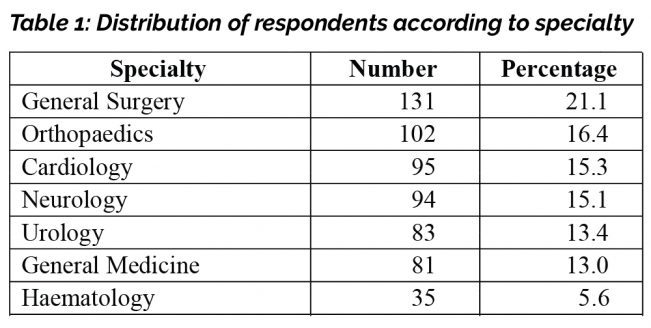
Patients attending the general surgery clinics comprised the highest number of respondents [131 (21%)] and haematology clinic patients comprised the least number of respondents [35 (6%)].
Demographic characteristics – Age, gender, ethnicity
There were 105 (17%) respondents between the ages of 18-35 years, 264 (42%) in the 36-60 years-group and 252 (41%) respondents were older than 60 years. Overall, 328 (53%) respondents were female. By ethnicity, African and East Indian descent patients were distributed equally, 275 (44%) and 278 (45%) respectively, and the remaining 68 (11%) belonged to mixed ethnic groups.
Demographic characteristics – Educational level and income
In terms of educational level, 302 (50%) were educated up to the primary level, 234 (38%) to the secondary level and 85 (12%) received tertiary education. Figure 1 shows the distribution of income of the respondents and the vast majority 505 (81%) of respondents earned lower than TT$ 4000 (US$ 625) per month.

Pain characteristics
When asked if they were currently experiencing pain, 427 (69%) of the 621 respondents indicated that they did suffer from pain. Of these, 76 patients (13% of the whole cohort) experienced acute pain, while 351 patients experienced pain lasting for more than 3 months, and thus the overall prevalence of chronic pain (in the whole cohort of 621 patients) was 56%. This distribution is shown in Figure 2.

Of the 351 patients who had chronic pain, Hospital III had the highest prevalence 150 (43%), while it was 95 (27%) in Hospital I and 106 (30%) in Hospital 2 (p<0.001).
The distribution of the intensity of the chronic pain as described by the respondents on the Numeric Rating Scale (NRS) of 1-10 is shown in Figure 3. Most patients scored their pain in the range of 5-10; 74 (21%) patients gave a score of 10, while 70 (20%) patients chose 8 as the pain score.

With respect to the location of chronic pain, although there was a wide distribution of pain throughout different parts of the body, pain in the lower limbs, back, chest and abdomen were the most commonly affected locations. When queried about the nature of the chronic pain, 154 (44%) patients described the pain as sharp and 130 (37%) as aching. Descriptions such as burning, stabbing and squeezing were less frequent.
As regards to the treatment the patients were currently receiving from the outpatient clinics for chronic pain, 319 of the 351 patients (90%) answered that they were being treated with analgesic medications. Surgical interventions were employed in 21 (6%) and physiotherapy was employed in 11 (4%) of patients.
Impact of chronic pain
Respondents were given six statements that were related to the impact of their chronic pain on their livelihood and asked to respond in a 5-point Likert Scale, which ranged from ‘strongly agree’ to ‘strongly disagree’. Table 1 shows the denomination and frequency of responses for each statement. As shown in the table, 81% of the respondents felt that chronic pain affected their quality of life and 64% agreed that pain affected their life financially; 82% were of the opinion that the chronic pain did affect their day-to-day activities. Also, 32% of respondents felt that the treatment they were currently receiving did not improve their pain and were not satisfied with the current treatment. Nearly half (47%) agreed that may visit private institutions in future for pain relief.
With respect to alternative treatment for pain, 225 (64%) responded that did not seek any. Of the remaining 126 (36%), 97 (77%) used over-the-counter herbal remedies, 22 (17%) had alternate medical therapy, and 7 (6%) chose acupuncture for alleviating their pain.
Factors associated with pain
Respondents of East Indian descent had a higher prevalence of chronic pain compared to African descent and mixed ethnicity. By gender, females had a higher prevalence of chronic pain than males. Also, the prevalence of chronic pain was higher in the ‘36-60’ age-group, compared to other age groups. Patients belonging to surgical clinics also had a higher prevalence of pain, compared to medical clinics. The details are shown in Table 2. There were no statistically significant differences between different educational levels and monthly income levels and the prevalence of pain (p=0.52 and p=0.73 respectively).

Discussion
The most salient findings of this study are the high prevalence and severe intensity of pain in adult patients attending the outpatient clinics of the major hospitals in Trinidad.
The American Academy for Pain Management suggested that over 1.5 billion people in the world suffer from pain [21]. The overall prevalence of chronic pain in the general population was reported to be 12% in Spain, Ireland, and the UK, 30% in Norway, Poland, and Italy, and 12% in Hong Kong adult population [3, 22].
Although these findings may be in the general population, there is a high prevalence of pain in the hospital settings also. A study from Italy showed a 63% prevalence of moderate intensity pain and 8% high-intensity pain in Internal Medicine patients [23]. Other published studies have reported the prevalence of pain ranging from 33% to 59 % in hospitalized as well as outpatients [15, 24-26]. This trend of high prevalence of pain in hospital patients may be true in Trinidad also but has been unrecognized so far.
With respect to demographics, in the present study, females had a higher prevalence of chronic pain, which has been reported in many studies [27-29]. Women have lower pain threshold and may experience more pain compared to males, and are at increased risk for developing chronic pain [30]. Many factors such as genotypes, sex hormones, stereotyped cultural beliefs are proposed factors that may play a role in sex difference in the perception of pain [31].
The present study found a higher prevalence of chronic pain in surgical patients when compared to medical patients, similar to a previous report which identified surgery as a major risk factor for chronic pain [32]. However, another study found no difference between medical and surgical patients [25].
The present study did not find a significant relationship between the prevalence of chronic pain and socio-economic factors such as educational level and monthly income. In contrast, a previous study reported that lower socio-economic classes did, in fact, have higher proportions of chronic pain patients [11].
Also in the present study, more than 40% of patients ranked their pain’s severity on the higher end (5-10) of the Numerical Rating Scale, while the Italian hospital-setting study reported a pain score of NRS ≥ 7 in 8% of the Internal Medicine patients [23].
With respect to the location of the chronic pain, the lower limbs and back were the most commonly afflicted anatomical parts. This is a common finding in many previous reports. Back pain was the leading category of pain in the European study as well as the report from the American Academy of Pain Management [3, 21].
Also in the present study, 81% indicated that their pain affected their quality of life. This is comparable to a study from Canada, which also stated that chronic pain impacted on the patients’ quality of life, disturbed their rest-time and caused unstable mindsets [9].
Chronic pain can be debilitating and can affect patients’ mobility, which may, in turn, affect their employment and income levels. This has been affirmed by a previous report, which indicated that there is a cost related to chronic pain [33]. The cost may be either directly due to factors such as the loss of productivity due to time off from work and reduced work efficiency, or loss of skills if people are forced to reduce their hours or stop working altogether [33].
In addition, the present study found that 40% of the adult patients attending the clinics were above 60 years, 81% earned <US$ 625 per month and half of the patients attained only primary school education. This may suggest that the majority of the persons utilizing the public healthcare system belonged to the so-called ‘economically dependent’ section of society. Hence, a high prevalence of chronic pain in such patients may very well lead to further economic strain creating a vicious cycle. There is an urgent need to break this cycle, by addressing their pain optimally within the public healthcare system.
Although 90% of respondents received analgesics, 33% responded that they did not have satisfactory pain relief. This is comparable to the European study, where an average of 40% of patients was found not satisfied with the treatment they were receiving [3]. This dissatisfaction would have been the reason for more than a third of respondents seeking alternative forms of treatment including herbal remedies in the present study.
It is noteworthy that 17% chose ‘not sure’ as the response for the statement ‘if they were satisfied with the treatment currently receiving’. This may suggest that there could have been a ‘social-desirability’ bias, implying that the patients might have chosen this response not to reflect badly on the health-providers of the hospitals they were attending.
The strengths of the current study are the relatively larger sample size, with a wider coverage of all hospitals, personally administered questionnaire and minimization of errors in capturing data. The limitations include purposive sampling, targeting outpatient clinic patients, which could have been the reason for the higher prevalence of chronic pain. Nevertheless, the fact remains that even in this group of the population, pain needs to be addressed, since they were not getting relieved by conventional treatment.
In summary, chronic pain was highly prevalent in adult patients attending the outpatient clinics of the major hospitals in Trinidad. Older age, female gender, East Indian ethnicity, and surgical conditions seemed to be the predisposing factors for a higher prevalence of pain.
There is a need for establishing protocols for appropriately managing acute and chronic pain in hospitals. In surgical patients, diligent implementation of multimodal and preemptive analgesia may prevent the development of chronic pain. Establishing dedicated pain management clinics in the public healthcare system of Trinidad & Tobago may be necessary to effectively treat common citizens with chronic pain, who may not be able to afford private healthcare.

References
1. Seattle: International Association for the Study of Pain. C2012 [updated 2012 May 22; cited 2012 July 3]. Available from www.iasp-pain.org
2. Treede R-D, Winfried Rief W, Antonia Barke A, et al. A classification of chronic pain for ICD-11. Pain. 2015; 156(6): 1003-7.
3. Breivik H, Collett B, Ventafridda V, Cohen R, Gallacher D. Survey of chronic pain in Europe: prevalence, impact on daily life, and treatment. Eur J Pain 2006;10: 287.
4. Goldberg DS, Summer JM. Pain as a global public health priority. BMC Public Health 2011;11: 770.
5. Gureje O, von Korff M, Kola L, Demyttenaere K, He Y, Posada-Villa J, Lepine JP, Angermeyer MC, Levinson D, de Girolamo G, Iwata N, Karam A, Borges GLG, de Graaf R, Browne MO, Stein DJ, Haro JM, Bromet EJ, Kessler RC, Alonso J. The relation between multiple pains and mental disorders: results from the World Mental Health Surveys. Pain 2008;135: 82–91.
6. Institute of Medicine (IOM). Relieving pain in America: a blueprint for transforming prevention, care, education, and research. Washington, DC: The National Academies Press, 2011.
7. Koleva D. Pain in primary care: an Italian survey. Eur J Public Health 2005;15: 475–9.
8. Mäntyselkä P, Kumpusalo E, Ahonen R, Kumpusalo A, Kauhanen J, Viinamäki H, Halonen P, Takala J. Pain as a reason to visit the doctor: a study in Finnish primary health care. Pain 2001;89: 175–80.
9. Reitsma ML, Tranmer JE, Buchanan DM, Vanderkherkhof Eg. The prevalence of chronic pain and pain-related interference in the Canadian population from1994- 2008. Chronic Diseases and Injuries in Canada 2011; 31(4):157-64.
10. Dominick C, Blyth F, Nicholas M. Patterns of chronic pain in the New Zealand Population. The New Zealand Medical J 2011; 124(1337): 63-7.
11. Liberman O, Freud T, Peleg R, Keren A, Press Y. Chronic pain and geriatric syndromes in community-dwelling patients aged ≥65 years. J Pain Res. 2018;11: 1171-80.
12. Loving S, Thomsen T, Jaszczak P, Nordling J. Female chronic pelvic pain is highly prevalent in Denmark. A cross-sectional population-based study with randomly selected participants. Scand J Pain. 2017; 5(2): 93-101.
13. Salomon L, Tcherny-Lessenot S, Collin E, Coutaux A, Levy-Soussan M, Legeron MC, et al. Pain prevalence in a French teaching hospital. J Pain Symptom Manage. 2002; 24(6): 586-92.
14. Costantini M, Viterbori P, Flego G. Prevalence of pain in Italian hospitals: results of a Regional Cross-sectional Survey. J Pain Symptom Manage. 2002; 23(3): 221-30.
15. Strohbuecker B, Mayer H, Evers G, Sabatowski R. Pain prevalence in hospitalized patients in a German University teaching hospital. J Pain Symptom Manage. 2005; 29(5): 498-506.
16. Sawyer J, Haslam L, Daines P, Stilos K. Pain prevalence study in a large Canadian Teaching Hospital. Round 2: Lessons Learned? Pain Manage Nurs. 2010; 11(1): 45-55.
17. Wadensten B, Fröjd C, Swenne CL, Torsten G, Gunningberg L. Why is pain still not being assessed adequately? Results of a pain prevalence study in a university hospital in Sweden. J Clin Nurs. 2011; 20(5-6): 624-34.
18. Perkins FM, Kehlet H, Chronic pain as an outcome of surgery. A review of predictive factors. Anesthesiology. 2000; 93(4): 1123-33.
19. Macrae WA. Chronic post-surgical pain: 10 years on. Br J Anaesth, 2008. 101(1): p. 77-86.
20. Searle RD, Simpson KH. Chronic Post-surgical Pain. Cont Edu Anaesth Crit Care & Pain. 2010; 10(1): 12-14.
21. Pleis JR, Ward BW, Lucas JW. Summary health statistics for U.S. adults: National Health Interview Survey, 2009. National Center for Health Statistics. Vital Health Stat. 2010.
22. Ng KF, Tsui SL, Chan WS. Prevalence of common chronic pain in Hong Kong adults. Clin J Pain. 2002; 18(5): 275-81.
23. Fabbian F, De Giorgi A, Pala M, Menegatti AM, Gallerani M, Manfredini R. Pain Prevalence and Management in an Internal Medicine Setting in Italy. Pain Research and Treatment. Volume 2014, Article ID 628284, (open access) http://dx.doi.org/10.1155/2014/628284
24. Conway Morris A, Howie N. Pain in medical inpatients: an under-recognised problem? J R Coll Physicians Edinb. 2009; 39(4): 292-5. doi: 10.4997/JRCPE.2009.401.
25. Rockett MP, Simpson G, Crossley R, Blowey S. Characteristics of pain in hospitalized medical patients, surgical patients, and outpatients attending a pain management centre. Br J Anaesth. 2013; 110(6): 1017-23. doi: 10.1093/bja/aet007.
26. Whelan CT, Jin L, Meltzer D. Pain and satisfaction with pain control in hospitalized medical patients: no such thing as low risk. Arch Intern Med. 2004; 164(2): 175-80.
27. Paller CJ, Campbell CM, Edwards RR, Dobs AS. Sex-based differences in pain perception and treatment. Pain Med. 2009;10(2): 289-99. doi: 10.1111/j.1526-4637.2008.00558.x. Epub 2009 Jan 16.
28. Kvachadze I, Tsagareli MG, Dumbadze Z. An overview of ethnic and gender differences in pain sensation. Georgian Med News. 2015; (238): 102-8.
29. Pieretti S, Di Giannuario A, Di Giovannandrea R, Marzoli F, Piccaro G, Minosi P, Aloisi AM. Gender differences in pain and its relief. Ann Ist Super Sanita. 2016; 52(2): 184-9. doi: 10.4415/ANN_16_02_09.
30. Tschugg A, Löscher WN, Hartmann S, Neururer S, Wildauer M, Thomé C. Gender Influences Radicular Pain Perception in Patients with Lumbar Disc Herniation. J Womens Health (Larchmt). 2015; 24(9): 771-6. doi: 10.1089/jwh.2014.5108. Epub 2015 Jun 24.
31. Bartley EJ, Fillingim RB. Sex differences in pain: a brief review of clinical and experimental findings. Br J Anaesth. 2013; 111(1): 52-8. doi: 10.1093/bja/aet127.
32. Crombie IK, Davies HT, Macrae WA. Cut and thrust: antecedent surgery and trauma among patients attending a chronic pain clinic. Pain 1998;76: 167–71.
33. Toth C, Lander J, Wiebe S. The prevalence and impact of chronic pain with neuropathic pain symptoms in the general population. Pain Med. 2009;10(5): 918-29.