
E Melki1, H Fares1, A Khaddam2, R Khaddam2
1 Department of General Surgery, Clinique Saint-Paul, Fort-de-France, Martinique, FWI
2 Cardiology Clinic, CSM, Fort-de-France, Martinique, FWI
Corresponding Author
Emile Melki1
Department of Obstetrics and Gynaecology
Clinique Saint-Paul 4 rue des Hibiscus 97200 Fort-de-France, Martinique, FWI
[email protected]
DOAJ: 181417c375b84231a67c4e5cc707786b
DOI: https://doi.org/10.48107/CMJ.2022.06.002
Copyright: This is an open-access article under the terms of the Creative Commons Attribution License which permits use, distribution, and reproduction in any medium, provided the original work is properly cited.
©2022 The Authors. Caribbean Medical Journal published by Trinidad & Tobago Medical Association.
ABSTRACT
Background
Endometriosis is a common disorder in women of childbearing age. Standard medical and surgical treatments are not always satisfactory. Shockwave therapy has been suggested as a possible novel treatment. There are no clinical data however to support this approach. This article describes the research protocol for a pilot interventional trial aiming to evaluate transvaginal low intensity shockwave therapy in women with endometriosis.
Methods
Adult women (anticipated N = 64) suffering from endometriosis will be recruited in a general gynaecology clinic and randomly allocated in a 1:1 ratio to an intervention group and a control group (parallel group design). The intervention group will receive 4 weekly sessions of transvaginal low intensity radial shockwave therapy. The control group will receive 4 sham procedures. The group allocation will be blinded to the patients but not to caregivers or data analysts (single blinded). Assessment will be carried at 1, 3 and 6 months. The primary endpoint is the visual analogue score for pelvic pain (dysmenorrhea, chronic pelvic pain, dysuria, dyschezia) and the deep dyspareunia score.
Conclusion
This prospective monocentric single blinded randomised controlled pilot trial will assess transvaginal low intensity shockwave therapy as a novel treatment for endometriosis.
KEYWORDS: Endometriosis; Pelvic pain; Dysmenorrhea; Dyspareunia; Shockwave Therapy.
INTRODUCTION
Background
Endometriosis is an inflammatory condition characterized by lesions of endometrial-like tissue outside of the uterus and is associated with pelvic pain and infertility.1 Prevalence is estimated at 10% to 15% of women of reproductive age and 70% of women with chronic pelvic pain worldwide.2 Epidemiological data in the Caribbean are scarce, with an estimated prevalence of 4 % in Puerto Rico in one study, underdiagnosis being likely.3 Symptoms include dysmenorrhea, dyspareunia, bladder and rectal pain that can severely alter quality of life. Although many treatment options are available and effective, a subset of patients does not benefit from standard treatment. It is estimated that 11% to 19% of women with endometriosis derive no pain relief at all from medical therapy.4 Some patients are ineligible to hormone therapy (history of venous thrombosis, history of oestrogen and progesterone receptor-positive cancer, history of meningioma for example). Surgery, especially excision of deep infiltrating endometriosis (DIE) can be challenging, and complications rates can be high. Major complications after colorectal segmental resection of bowel endometriosis occurs in 11 % of patients.5 Moreover, long‐term urinary and digestive side effects are common following surgery.6-7 There is a need for new, effective and safe therapeutic methods. High intensity focalised ultrasound (HIFU) and radiofrequency ablation (RFA) are being evaluate.8-9-10 Symptomatic treatment by transcutaneous electrical nerve stimulation (TENS) is also a promising technique.11 Shockwave therapy (SWT) has been suggested as a novel approach to treat endometriosis.12
A shockwave is a form of acoustic energy resulting from a sudden and intense change in pressure, which produces waves of energy through elastic mediums like human soft tissue or bone. High intensity focused shockwaves are used to obtain a disruptive effect (as in lithotripsy), whereas low intensity radial or focused shockwaves are applied to achieve pain relief via neuromodulatory, antioxidant and anti-inflammatory effects. This trial aims to evaluate the latter approach. In chronic conditions pain threshold is progressively lowered. Smaller nociceptive stimuli are therefore transmitted by neural pathways, and then processed and amplified by the central nervous system. The specific role of myofascial pain in endometriosis has been highlighted and could explain standard medical and surgical treatment failure in some patients.13 By targeting pelvic myofascial trigger points with SWT, the nociceptive sensitisation feed-back loop could be interrupted. Shockwaves may induce nitric oxide (NO) synthesis by way of endothelial nitric oxide synthase release.14 NO is a modulator of inflammatory process and can down regulate activation of neutrophils, macrophages, mast cells, endothelial cells, and platelets.15 This is of importance as inflammation is now considered a cornerstone of the disease. The peritoneal fluid of women with endometriosis has been found to contain abnormally high levels of numerous pro-inflammatory cytokines like IL-1, IL-8 and TNF-α.16 NO is also a potent free radical scavenger. The ability of NO to scavenge superoxide anion (O2–) has been documented both in vitro and in vivo.15 Oxidative stress is part of the toxic molecular environment of endometriosis and has been linked to fertility impairment in this disease.17 In clinical experience SWT proved successful in musculoskeletal diseases with a favourable tolerance profile.18-19-20-21-22-23 Good outcomes have also been achieved in chronic pelvic pain syndrome/chronic prostatitis in males (CPPS/CP).24-25 However, experience in females is very limited. Meneghini et al. applied focused low-energy extracorporeal SWT to 3 patients with CPPS. One patient only was premenopausal, her symptoms consisting of anal and gluteal pain, worsening during menstruation (no clinical or imaging evidence of endometriosis is mentioned).26 After four weekly sessions of SWT, assessment at one week did not show any improvement. At eight months follow-up pain scores were variable during the day but no analgesic drugs were taken. Of the two other post-menopausal patients, the first showed a clear improvement while the other’s symptoms were unchanged. Tung et al.27reported a case of female chronic perineal pain successfully treated by focused low-energy extracorporeal SWT. A 51-year-old woman (menopausal status unknown) developed scar tissue pain after removal of a vulvo-vaginal non-endometriotic inclusion cyst. Pain scores were significantly reduced after 11 monthly SWT sessions. These are case reports with no control groups, therefore a placebo effect cannot be ruled out. Xing et al. published a randomised trial assessing extracorporeal radial SWT in primary dysmenorrhea without organic lesions.28 SWT was applied to abdominal « acupuncture points » in the follicular phase (Group A, N=15) or the luteal phase (Group B, N=14). The control group (Group C, N=15) received heat patch application to the same points. Pain severity (VAS) was significantly lower in the three groups after treatment but the reduction was greater in the SWT groups, without difference between them (induced relative changes in Groups A -53.8 %, in Group B -59.3 %, in Group C -18.7 %). Another small, randomised trial of extracorporeal radial SWT in primary dysmenorrhea is underway. SWT will be applied to prespecified abdominal myofascial trigger points and outcome assessment will include a brain functional MRI.29
We still lack data regarding SWT as a treatment of pelvic pain in females in general, and in endometriosis patients in particular. Furthermore, there are no published studies on transvaginal SWT. Radial shockwave energy decreases by square relative to the penetration depth through biological tissue.30 Transabdominal or transperineal applications are affected by morphotype variations, whereas the transvaginal route of administration could be beneficial by allowing a more direct access to pelvic anatomical structures.
Research objective
To evaluate the feasibility, tolerance and efficacy of transvaginal low intensity SWT as a treatment for endometriosis.
METHODS
Trial design
This is prospective, monocentric, randomised [1:1], single-blinded, placebo-controlled, parallel-group study (refer to Figure 1).
Participants
All participants will be given clear verbal and written information about the trial and will give written consent. The rationale, expected risks and benefits of this novel treatment will be expressed in a simple way. Consent can be withdrawn at any moment by the participants, leading to withdrawal from the trial. Surgery or ART can be offered to participants if deemed necessary, leading to withdrawal from the trial.
Baseline characteristics will be collected according to protocol guidelines (Figure 2).
Figure 2: Baseline Characteristics
Age in years
-18-29
-30-45
-46 or older
Body Mass Index (BMI)
-less than 18.5
-18.5-24.9
-25-29.9
-30 or greater
Parity
-para 0
-para 1
-para 2 or more
Endometriosis localisation
-Superficial peritoneal
-Ovarian endometrioma
-DIE
History of surgery for endometriosis
-Yes
-No
Menstrual cycle pattern
-complete induced amenorrhea
-irregular cycle pattern
-regular cycle
Ongoing treatment
-oral progestogens or oestro-progestogens
-GnRH analogues
-progestogen-releasing IUDs
Baseline pain level for dysmenorrhea
-VAS less than 5
-5-7
-7 or greater
Baseline pain level for chronic pelvic pain
-VAS less than 5
-5-7
-7 or greater
Baseline pain level for dysuria
-VAS less than 5
-5-7
-7 or greater
Baseline pain level for dyschezia
-VAS less than 5
-5-7
-7 or greater
Deep dyspareunia score
-0
-1
-2
-3
Inclusion criteria
Women aged 18 years and older, with clinical symptoms and imaging findings on ultrasound scan and MRI confirming the diagnosis of endometriosis, will be recruited by referral. Gynaecologists, general practitioners and midwives in Martinique will be informed of the trial and invited to refer patients for possible inclusion. Ovarian endometriomas, superficial and deep endometriosis meet the inclusion criteria. Histological confirmation is not mandatory, as French guidelines do not support the need for direct visualisation or pathological evidence to ascertain the diagnosis in routine practice.31 In a trial setting this would be certainly desirable but warranting laparoscopy would raise difficult ethical and practical questions and restricting the trial to operated patients would drastically limit recruitment as well as likely introduce bias. Medical treatment (oral progestogens or oestro-progestogens, GnRH analogues, progestogen-releasing IUDs) should be deemed unsatisfactory thus warranting the intervention but should not be discontinued during the trial. Pain-relief medication can be prescribed as recommended by standard of care practice.
Exclusion criteria
Women unable to give consent, to understand written and verbal French, or to comply with follow-up.
Virgin women
Pregnant women (a pregnancy test should be performed 72 hours at least before each session), women planning pregnancy or undergoing fertility treatment.
Post-partum period until 6 weeks after delivery.
Any vulvo-vaginal condition contraindicating the vaginal route (vaginismus, radiation-induced atrophy etc.).
History of vesico or recto-vaginal fistula.
History of obstetrical perineal tear of grade 3 or 4.
History of segmental rectal resection with mechanical anastomosis, shaving or discoid resection.
History of another pelvic surgery in the last 6 months.
Women with ureterohydrephrosis warranting ureteral stenting and surgical treatment.
Women with ongoing uro-genital infection.
ESSURE® tubal contraceptive implants.
Study setting
Monocentric (Clinique Saint-Paul, private hospital in Fort-de-France, Martinique, French West Indies). This is a general hospital (secondary health care centre) with a general gynaecology clinic. It is a contracted institution under French public insurance regulation. The hospital does not have a local research ethics committee. The trial will be submitted for authorisation to the regional ethics committee (Comité de Protection des Personnes CPP Sud-Ouest et Outre-Mer III, Bordeaux) and to the regional health agency in Martinique (Agence Regionale de Santé). A local Monitoring Board comprised of senior attending physicians will be created to supervise the trial implementation and safety A dedicated telephone number will be given to participants to report any adverse event. Medical support will be available at any moment.
Intervention
Transvaginal low intensity SWT will be applied on a weekly basis for 4 weeks, using a Masterpuls® One system with a Sparrow® handpiece (Storz Medical, Switzerland). Sterilisation of the probe will be performed between interventions according to hospital protocols. Each session will consist of a systematic application of radial shockwaves at the level of the cervix and at the mid vaginal level. Additional targeted applications will be directed to the vaginal fornices or vaginal walls using biofeedback (trigger point localization by the probe pressure). At each level the parameters will be set at 2 bars, 720 pulses, 5 Hz, for a duration of 2 minutes. A sham procedure will be carried out in the control group (blinded to the patient only). The same handpiece will be used with the same protocol as in the intervention group but without shockwave output. The typical sound signature of SWT should be replicated during the sham procedure.
Outcomes
Clinical evaluation will be carried before treatment, at 1 month, 3 months and 6 months using validated questionnaires. Ultrasound scan and MRI assessment will be carried at 6 months.
Primary endpoint:
Pain level in dysmenorrhea (in cycling women), chronic pelvic pain, dysuria and dyschezia will be assessed using the Visual Analogue Scale (VAS) (Figure 3).
Dyspareunia (in sexually active women) will be assessed using the deep dyspareunia scale (DDS) (11)
0 = no pain during intercourse; 1 = mild pain; 2 = moderate pain; 3 = intense pain which requires the interruption of intercourse.
To minimise recall bias, dysmenorrhea level will be assessed on the last menstrual period, chronic pelvic pain, dysuria and dyschezia on the last week, and dyspareunia on the last intercourse before each evaluation.
Secondary endpoints
Quality of life : French version of EHP-5(32) (Figure 5).
Figure 5 : FSFI questionnaire, English and French versions (Wylomanski et al.) 33
All items are rated 0 to 5
- Over the past 4 weeks, how often did you feel sexual desire or interest?
Au cours des 4 dernières semaines, avez-vous ressenti un désir sexuel?
- Over the past 4 weeks, how would you rate your level (degree) of sexual desire or interest?
Au cours des 4 dernières semaines, quel a été le niveau (degré) de votre désir sexuel
- Over the past 4 weeks, how often did you feel sexually aroused (“turned on”) during sexual activity or intercourse?
Au cours des 4 dernières semaines, vous êtes-vous sentie excitée sexuellement pendant une activité sexuelle ou un rapport sexuel?
- Over the past 4 weeks, how would you rate your level of sexual arousal (“turn on”) during sexual activity or intercourse?
Au cours des 4 dernières semaines, quel a été votre niveau (degré) d’excitation au cours d’une actvité ou d’un rapport sexuel?
5.Over the past 4 weeks, how confident were you about becoming sexually aroused during sexual activity or intercourse?
Au cours des 4 dernières semaines, a quel point avez-vous été sûre de votre capacité à être excitée au cours d’une activité ou d’un rapport sexuel?
- Over the past 4 weeks, how often have you been satisfied with your arousal (excitement) during sexual activity or intercourse?
Au cours des 4 dernières semaines, avez-vous été satisfaite de votre degré d’excitation pendant une activité ou un rapport sexuel?
- Over the past 4 weeks, how often did you become lubricated (“wet”) during sexual activity or intercourse?
Au cours des 4 dernières semaines, votre vagin était lubrifé (humide) au cours d’une activité ou d’un rapport sexuel?
- Over the past 4 weeks, how difficult was it to become lubricated (“wet”) during sexual activity or intercourse?
Au cours des 4 dernières semaines, à quel point vous a-t-il été difficile d’avoir le vagin lubirifé (humide) au cours d’une activité ou d’un rapport sexuel?
- Over the past 4 weeks, how often did you maintain your lubrication (“wetness”) until completion of sexual activity or intercourse?
Au cours des 4 dernières semaines, la lubrification (humidité) de votre vagin a-t-elle duré jusqu’à la fin d’une activité ou d’un rapport sexuel?
- Over the past 4 weeks, how difficult was it to maintain your lubrication (“wetness”) until completion of sexual activity or intercourse?
Au cours des 4 dernières semaines, vous a-t-il été difficile de conserver la lubrification (humidité) de votre vagin jusqu’à la fin d’une activité ou d’un rapport sexuel?
- Over the past 4 weeks, when you had sexual stimulation or intercourse, how often did you reach orgasm (climax)?
Au cours des 4 dernières semaines, lorsque vous avez été stimulée sexuellement ou que vous avez eu un rapport sexuel, avez-vous atteint l’orgasme?
- Over the past 4 weeks, when you had sexual stimulation or intercourse, how difficult was it for you to reach orgasm (climax)?
Au cours des 4 dernières semaines, lorsque vous avez eu un rapport sexuel, à quel point vous a-t-il été difficile d’atteindre l’orgasme?
- Over the past 4 weeks, how satisfied were you with your ability to reach orgasm (climax) during sexual activity or intercourse?
Au cours des 4 dernières semaines, à quel point avez vous été satisfaite de votre capacité à atteindre l’orgasme pendant une activité sexuelle ou un rapport sexuel?
- Over the past 4 weeks, how satisfied have you been with the amount of emotional closeness during sexual activity between you and your partner?
Au cours des 4 dernières semaines, à quel point avez-vous été satisfaite de votre relation affective avec votre partenaire pendant une activité sexuelle?
- Over the past 4 weeks, how satisfied have you been with your sexual relationship with your partner?
Au cours des 4 dernières semaines, à quel point avez-vous été satisfaite de votre relation avec votre partenaire d’un point de vue sexuel?
- Over the past 4 weeks, how satisfied have you been with your overall sexual life?
Au cours des 4 dernières semaines, à quel point avez-vous été satisfaite de votre vie sexuelle en général?
- Over the past 4 weeks, how often did you experience discomfort or pain during vaginal penetration?
Au cours des 4 dernières semaines, avez-vous ressenti une gêne ou une douleur pendant la pénétration vaginale?
- Over the past 4 weeks, how often did you experience discomfort or pain following vaginal penetration?
Au cours des 4 dernières semaines, avez-vous ressenti une gêne ou une douleur après la pénétration vaginale?
- Over the past 4 weeks, how would you rate your level (degree) of discomfort or pain during or following vaginal penetration?
Au cours des 4 dernières semaines, quel a été votre niveau (degré) de gêne ou de douleur pendant ou après la pénétration vaginale?
Sexual function : French version of FSFI questionnaire (Figure 6).33
Use of pain relief medication (type and frequency per week).
Imaging results at 6 months: improvement, stability, worsening of lesions as assessed by a specialised radiologist.
Tolerance will be assessed by the analysis of adverse events (pelvic, vulvo-vaginal, urinary, digestive or other events).
Sample size
Considering a small estimated effect size of 0.2, the recommended sample size for a pilot trial is 50 individuals (25 in each group) to meet the 90% statistical value and the 5% significance level.34 As we expect a 20% drop-out rate, the sample size was finally determined to be 64 participants (32 per group). The results of this pilot study will facilitate the calculation of an appropriate sample size for further randomised clinical trials.
Trial monitoring
No interim analysis is planned.
Adverse events (AE) will be categorised as mild, moderate or major.
Mild AE include: vulvo-vaginal irritation, vaginal discharge, pelvic discomfort.
Moderate AE include: vulvo-vaginal or pelvic pain (over baseline), lower urinary tract infection, constipation or diarrhoea.
Major AE: any event needing hospitalisation, upper urinary tract infection, upper genital tract infection, urinary retention, intestinal occlusion, fistula formation.
Any major medical event during the trial will be submitted the Monitoring Board to assess potential causality. The board can exclude a participant or stop the trial at any moment if deemed necessary.
Randomisation
Patients will be allocated to the two groups in a 1:1 ratio using block randomisation with a computer-generated list of random numbers using block sizes of four. Allocation will be carried out by researchers in a separate location (AK and RK) and the allocation sequence will be concealed from the researchers (EM and HF) enrolling and assessing participants in sequentially numbered, opaque, sealed and stapled envelopes.
Blinding
Participants will be blinded to the allocation (single blinding). Intervention providers and investigators will not be blinded. Although the sham procedure in the control group will be made as realistic as possible, the unavoidable difference in sensory experience between the groups could lead to sub-optimal single blinding.
Statistical analysis
Analysis will be carried out on an intention-to-treat basis and will be performed using SPSS 23.0 statistical software (IBM SPSS Statistics, New York, USA). Lost to follow-up participants will be censored at the time of their last assessment. The distributed variables will be compared by using the student t test. Statistical analysis of continuous values will be carried through the independent samples t test. The Mann–Whitney U test and the χ2 test will be used for the comparison of quantitative data. P < .05 will be considered statistically significant.
Statistical analysis will be carried on the following subgroups:
Age in years (18-29, 30-45, 46 or older), Body Mass Index (BMI) (less than 18.5, 18.5-24.9, 25-29.9, 30 or greater), baseline pain level (VAS less than 5, 5-7, 7 or greater), endometriosis localisation (peritoneal, ovarian endometrioma, DIE), menstrual cycle pattern (complete induced amenorrhea, irregular cycle pattern, regular cycle), ongoing treatment (oral progestogens or oestro-progestogens, GnRH analogues, progestogen-releasing IUDs).
Trial duration
The trial will end after the final 6-month assessment of the last recruited participant.
Data management
A password-protected electronic database will be created. Participant information will be anonymised using study numbers. All researchers will have access to the database.
DISCUSSION
Efficacy and safety of SWT as a treatment for endometriosis have yet to be demonstrated. We believe a pilot human trial is ethically and scientifically acceptable, without prior animal experimentation, as this technique is widely used in other indications worldwide in standard clinical settings. The goal is primarily to validate the feasibility of a future larger trial by assessing tolerability, randomization acceptance and implementation, follow-up and evaluation. Although probably underpowered to detect a small difference between the two groups, collected data will help with future study designs (for example to determine sample sizes). Robust subgroup analysis will obviously need larger trials (comparison between DIE, superficial peritoneal endometriosis and ovarian endometrioma groups, comparison between different hormone therapy groups etc.). The lack of stratification according to baseline characteristics can introduce bias.
Technically, the choice of low intensity (equivalent to 0,09 mJ/mm2) and radial shockwaves aims to maximise tolerability and safety. In musculoskeletal applications the paradigm has progressively shifted from high-intensity focalised SWT to low intensity radial SWT, with no difference in outcomes.30 Keeping the energy level low is of paramount importance in the risk-benefit balance. High intensity energy application in the pelvis may induce necrosis and fistula formation.35 There is a case report of recto-uterine fistula after RFA of a uterine fibroid, and several reports of bowel perforation after HIFU for uterine fibroids and adenomyosis.36-37-38 Based on experience in other diseases, we believe the risk-benefit balance of transvaginal low intensity SWT is favourable compared to HIFU, RFA or indeed surgery but only properly designed and implemented trials can provide robust safety data.
The number of procedures (four at weekly intervals) is based on SWT literature, but it is in fact empirical and debatable. In musculoskeletal disease one to three SWT sessions at weekly intervals is considered standard clinical practice regardless of the underlying pathology.30 In CPPS/CP in males between four and eight weekly procedures were carried out.24-25 Meneghini et al. applied four weekly sessions in the treatment of CPPS in females.26 In Xing’s trial participants received two treatment sessions within one menstrual cycle over three cycles.28 Further studies are certainly necessary to specify the optimal number of procedures. Lower energy levels per procedure probably require more treatment sessions to obtain the same effect. 30
Ultrasound targeting of endometrial lesions is possible but remains operator-dependent, time-consuming and increases costs. Moreover « biofeedback targeting » in which the patient helps with the localisation of trigger points has demonstrated superiority over ultrasound targeting in musculoskeletal indications. 30Anaesthesia is best avoided as it has been shown in randomised trials that local anaesthesia reduces the effect of SWT.30 There is experimental evidence that SWT activates and sensitises primary afferent nociceptive C-fibres, and that both activation and sensitisation were prevented if local anaesthesia was applied.39
The transvaginal route is a novel approach to SWT application in females. It has theoretical biophysical advantages over transabdominal or transperineal routes (direct anatomical access to lesions, less energy loss at target, straightforward biofeedback loop) but can raise cultural or personal acceptability issues and is contraindicated in virgin women. The rectal route is an alternative, albeit with specific acceptability limits.
With respect to external validity, we believe the setting of this trial (general gynaecology clinic in a secondary health centre) is an asset, as it reflects « real life » experience of a majority of caregivers and patients, in contrast to specialised tertiary units. The technical expertise needed to perform the intervention requires a moderate amount of training and the equipment remains accessible to institutions even in low-income parts of the world.
Figure 1: Flow chart showing enrolment, allocation, follow-up and analysis
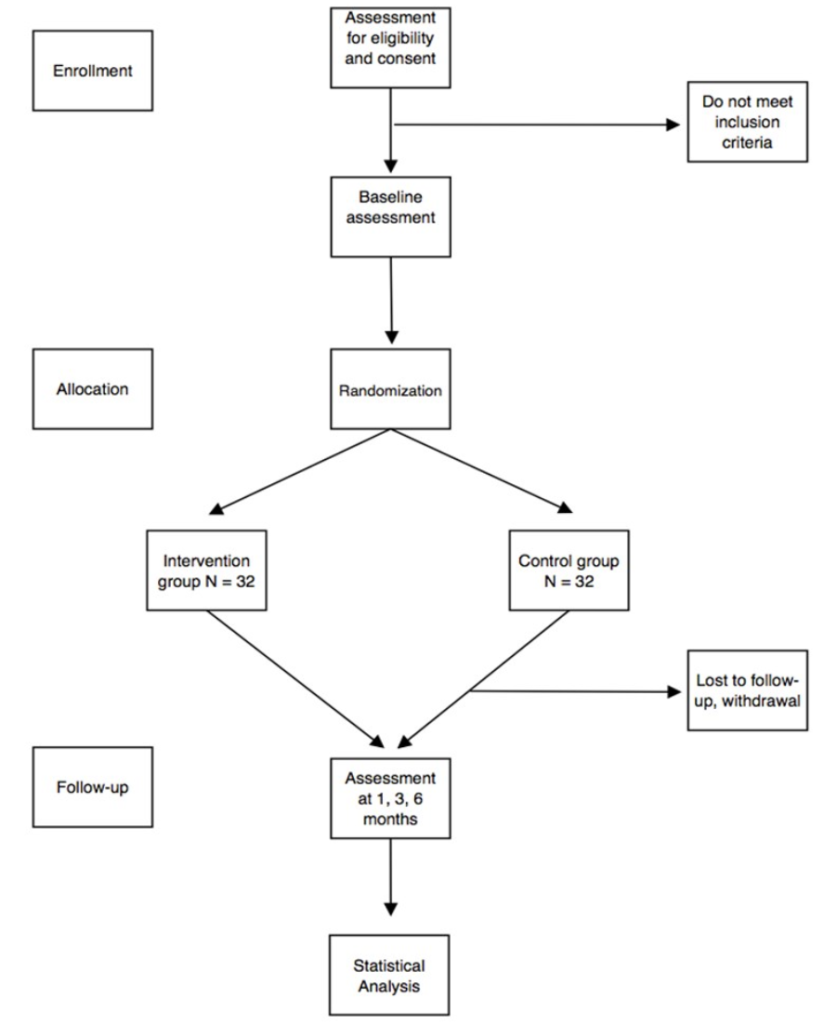
Figure 3: Visual Analogue Scale
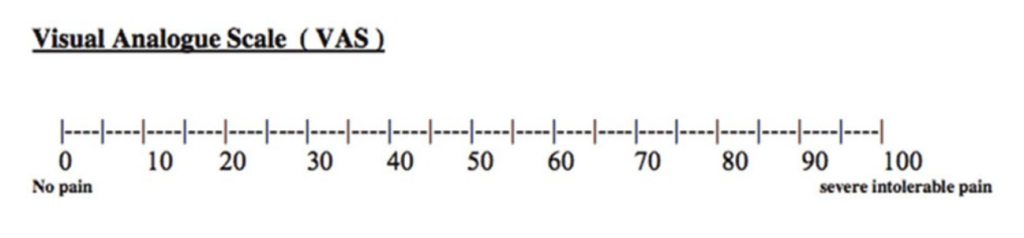
Figure 4 : EHP 5 questionnaire, English and French versions (Renouvel et al.) 32

Ethical Approval statement: This trial will be submitted before patient recruitment to the regional ethics committee (comité de protection des personnes CPP Sud-Ouest et Outre-Mer III, Bordeaux) and to the regional health agency (Agence Régionale de Santé Martinique). This trial will be registered in ClinicalTrials.gov.
Conflict of interest statement: The Authors declare that there is no conflict of interest.
Informed Consent statement: Written informed consent will be obtained from all subjects before enrolment. This trial will comply with the Declaration of Helsinki on ethical principles for medical research involving human subjects.
Funding statement: This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Author Contributions: EM researched literature, conceived the study and wrote the first draft of the manuscript. HF, AK and RK were involved in protocol development, manuscript review and editing. All authors approved the final version of the manuscript.
An early version of this article was posted (non-peer-reviewed) on the Centre for Direct Scientific Communication (CCSD) open archive website (https://hal.archives-ouvertes.fr/hal-03152988).
REFERENCES
- Johnson NP, Hummelshoj L, for the World Endometriosis Society Montpellier Consortium, Abrao MS, Adamson GD, Allaire C, et al,” Consensus on current management of endometriosis,”. Hum Reprod. 2013 Jun 1;28(6):1552–68.
- Parasar P, Ozcan P, Terry KL,” Endometriosis: Epidemiology, Diagnosis and Clinical Management,” Curr Obstet Gynecol Rep. 2017 Mar;6(1):34–41.
- Flores I, Abreu S, Abac S, Fourquet J, Laboy J, Ríos-Bedoya C,” Self-reported prevalence of endometriosis and its symptoms among Puerto Rican women,” Int J Gynecol Obstet. 2008;100(3):257–61.
- Becker CM, Gattrell WT, Gude K, Singh SS,”Reevaluating response and failure of medical treatment of endometriosis: a systematic review,” Fertil Steril. 2017 Jul;108(1):125–36.
- Cicco CD, Corona R, Schonman R, Mailova K, Ussia A, Koninckx PR,”Bowel resection for deep endometriosis: a systematic review,” BJOG Int J Obstet Gynaecol. 2011 Feb 1;118(3):285–91.
- Dubernard G, Rouzier R, David-Montefiore E, Bazot M, Daraï E,” Urinary complications after surgery for posterior deep infiltrating endometriosis are related to the extent of dissection and to uterosacral ligaments resection,” J Minim Invasive Gynecol. 2008 Apr;15(2):235–40.
- Roman H, Vassilieff M, Tuech JJ, Huet E, Savoye G, Marpeau L, et al,” Postoperative digestive function after radical versus conservative surgical philosophy for deep endometriosis infiltrating the rectum,” Fertil Steril. 2013 May;99(6):1695–704.
- Carrafiello G, Fontana F, Pellegrino C, Mangini M, Cabrini L, Mariani D, et al,” Radiofrequency ablation of abdominal wall endometrioma,” Cardiovasc Intervent Radiol. 2009 Nov;32(6):1300–3.
- Zhao L, Deng Y, Wei Q, Chen J, Zhao C,” Comparison of ultrasound-guided high-intensity focused ultrasound ablation and surgery for abdominal wall endometriosis,” Int J Hyperth Off J Eur Soc Hyperthermic Oncol North Am Hyperth Group. 2018 Sep 13;1–6.
- Dubernard G, Gelet A, Lafon C, Guillen N, Chavrier F, Chapelon J-Y, et al,” Transrectal high-intensity focused ultrasound as focal therapy for posterior deep infiltrating endometriosis,” Ultrasound Obstet Gynecol Off J Int Soc Ultrasound Obstet Gynecol. 2018;51(1):145–6.
- Mira TAA, Yela DA, Podgaec S, Baracat EC, Benetti-Pinto CL,”Hormonal treatment isolated versus hormonal treatment associated with electrotherapy for pelvic pain control in deep endometriosis: Randomized clinical trial,” Eur J Obstet Gynecol Reprod Biol. 2020 Dec; 255:134–41.
- Melki E,” Endometriosis treatment with shock waves: A novel approach,” Med Hypotheses. 2019 Mar; 124:114–7.
- Aredo JV, Heyrana KJ, Karp BI, Shah JP, Stratton P,” Relating Chronic Pelvic Pain and Endometriosis to Signs of Sensitization and Myofascial Pain and Dysfunction,” Semin Reprod Med. 2017 Jan;35(1):88–97.
- Mariotto S, de Prati AC, Cavalieri E, Amelio E, Marlinghaus E, Suzuki H,” Extracorporeal shock wave therapy in inflammatory diseases: molecular mechanism that triggers anti-inflammatory action,” Curr Med Chem. 2009;16(19):2366–72.
- Wallace JL,” Nitric oxide as a regulator of inflammatory processes,” Mem Inst Oswaldo Cruz. 2005 Mar;100 Suppl 1:5–9.
- Herington JL, Bruner-Tran KL, Lucas JA, Osteen KG,” Immune interactions in endometriosis,” Expert Rev Clin Immunol. 2011 Sep;7(5):611–26.
- Scutiero G, Iannone P, Bernardi G, Bonaccorsi G, Spadaro S, Volta CA, et al,” Oxidative Stress and Endometriosis: A Systematic Review of the Literature,” Oxid Med Cell Longev [Internet]. 2017 [cited 2018 Oct 22];2017. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5625949/
- GEZGİNASLAN Ö, GÜMÜŞ ATALAY S,” High-Energy Flux Density Extracorporeal Shock Wave Therapy Versus Traditional Physical Therapy Modalities in Myofascial Pain Syndrome: A Randomized-controlled, Single-Blind Trial,” Arch Rheumatol. 2019 Jun 25;35(1):78–89.
- Park KD, Lee WY, Park M, Ahn JK, Park Y,” High- versus low-energy extracorporeal shock-wave therapy for myofascial pain syndrome of upper trapezius,” Medicine (Baltimore) [Internet]. 2018 Jul 13 [cited 2020 Dec 22];97(28). Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6076058/
- Eftekharsadat B, Fasaie N, Golalizadeh D, Babaei-Ghazani A, Jahanjou F, Eslampoor Y, et al,” Comparison of efficacy of corticosteroid injection versus extracorporeal shock wave therapy on inferior trigger points in the quadratus lumborum muscle: a randomized clinical trial,” BMC Musculoskelet Disord [Internet]. 2020 Oct 19 [cited 2020 Dec 22];21. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7574569/
- Aktürk S, Kaya A, Çetintaş D, Akgöl G, Gülkesen A, Kal GA, et al,” Comparision of the effectiveness of ESWT and ultrasound treatments in myofascial pain syndrome: randomized, sham-controlled study,” J Phys Ther Sci. 2018 Mar;30(3):448–53.
- Wu Y-T, Chang C-N, Chen Y-M, Hu G-C,” Comparison of the effect of focused and radial extracorporeal shock waves on spastic equinus in patients with stroke: a randomized controlled trial,” Eur J Phys Rehabil Med. 2018 Aug;54(4):518–25.
- Walewicz K, Taradaj J, Dobrzyński M, Sopel M, Kowal M, Ptaszkowski K, et al,” Effect of Radial Extracorporeal Shock Wave Therapy on Pain Intensity, Functional Efficiency, and Postural Control Parameters in Patients with Chronic Low Back Pain: A Randomized Clinical Trial,” J Clin Med [Internet]. 2020 Feb 19 [cited 2020 Dec 26];9(2). Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7074373/
- Vahdatpour B, Alizadeh F, Moayednia A, Emadi M, Khorami MH, Haghdani S,” Efficacy of extracorporeal shock wave therapy for the treatment of chronic pelvic pain syndrome: a randomized, controlled trial,” ISRN Urol. 2013; 2013:972601.
- Zhang Z-X, Zhang D, Yu X-T, Ma Y-W,” Efficacy of Radial Extracorporeal Shock Wave Therapy for Chronic Pelvic Pain Syndrome: A Nonrandomized Controlled Trial,” Am J Mens Health. 2018 Nov 28;1557988318814663.
- Meneghini, A, Trevisan M, Lampropoulo E, Meneghini N,” Chronic pelvic pain syndrome in women. Review and preliminary results with low-energy extracorporeal shock wave therapy,” Pelviperineology. 2015;(34):60–6.
- Tung CW, Cheon WC, Tong A,” Novel treatment of chronic perineal pain in a woman by extracorporeal shock wave therapy: a case report and published work review,” J Obstet Gynaecol Res. 2015 Jan;41(1):145–8.
- Xing R, Yang J, Wang R, Wang Y,” Extracorporeal shock wave therapy for treating primary dysmenorrhea,” Medicine (Baltimore). 2021 Feb 5;100(5): e23798.
- Liu S, Wang L, Yang J,” Instant analgesic effect of radial extracorporeal shock wave therapy on primary dysmenorrhoea according to functional magnetic resonance imaging: study protocol for a randomised placebo-controlled trial,” Trials. 2020 Feb 11;21(1):164.
- Lohrer H, Nauck T, Korakakis V, Malliaropoulos N,” Historical ESWT Paradigms Are Overcome: A Narrative Review,” BioMed Res Int [Internet]. 2016 [cited 2018 Oct 22];2016. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4967434/
- HAS. Prise en charge de l’endométriose recommandation pour la pratique clinique [Internet]. Available from: https://www.has-sante.fr/upload/docs/application/pdf/2018-01/prise_en_charge_de_lendometriose_-_recommandations.pdf
- Renouvel F, Fauconnier A, Pilkington H, Panel P ,”Linguistic adaptation of the endometriosis health profile 5: EHP 5,”. J Gynecol Obstet Biol Reprod (Paris). 2009 Sep;38(5):404–10.
- Wylomanski S, Bouquin R, Philippe H-J, Poulin Y, Hanf M, Dréno B, et al,” Psychometric properties of the French Female Sexual Function Index (FSFI),” Qual Life Res Int J Qual Life Asp Treat Care Rehabil. 2014 Sep;23(7):2079–87.
- Whitehead AL, Julious SA, Cooper CL, Campbell MJ,” Estimating the sample size for a pilot randomised trial to minimise the overall trial sample size for the external pilot and main trial for a continuous outcome variable,” Stat Methods Med Res. 2016 Jun;25(3):1057–73.
- Jeong HJ, Kwon B-S, Choi YJ, Huh CY,” Rectouterine fistula after laparoscopic ultrasound-guided radiofrequency ablation of a uterine fibroid,” Obstet Gynecol Sci. 2014 Nov;57(6):553–6.
- Chen J, Chen W, Zhang L, Li K, Peng S, He M, et al,” Safety of ultrasound-guided ultrasound ablation for uterine fibroids and adenomyosis: A review of 9988 cases,” Ultrason Sonochem. 2015 Nov; 27:671–6.
- Hwang DW, Song HS, Kim HS, Chun KC, Koh JW, Kim YA,” Delayed intestinal perforation and vertebral osteomyelitis after high-intensity focused ultrasound treatment for uterine leiomyoma,” Obstet Gynecol Sci. 2017 Sep;60(5):490–3.
- Ko JKY, Cheung VYT,” Comment on: Delayed intestinal perforation and vertebral osteomyelitis after high-intensity focused ultrasound treatment for uterine leiomyoma,” Obstet Gynecol Sci. 2018 Mar;61(2):177–8.
- Klonschinski T, Ament SJ, Schlereth T, Rompe JD, Birklein F,” Application of local anesthesia inhibits effects of low-energy extracorporeal shock wave treatment (ESWT) on nociceptors,” Pain Med Malden Mass. 2011 Oct;12(10):1532–7.