
Ruchelle Brown Calvert1, Akshai Mansingh, Sharmella Roopchand-Martin, Praimanand Singh.
1Faculty of Sport, The University of the West Indies, Mona, Jamaica.
Corresponding Author:
Ruchelle Brown Calvert
Faculty of Sport
The University of the West Indies
Mona, Jamaica
Email: [email protected]
Copyright: This is an open-access article under the terms of the Creative Commons Attribution License which permits use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
To take an epidemiological look into hamstring injuries in Jamaican athletes presenting to the University of the West Indies (UWI) Sport Medicine Clinic between 2007 and 2016. The research focused on the contribution of certain demographics and types of sports and activities to the classification, recovery and recurrence of these injuries.
A retrospective chart review was conducted on all the athletes who presented to the UWI Sports Medicine Clinic between 2007 and 2016. An electronic data extraction sheet was used for data collection. The target population consisted of athletes from 13 to 25 years of age who participated in competitive sports at the time of injury.
Of the 125 dockets reviewed, 92 were males (73.6%), 30 were females (24%) and three were of unknown sex (2.4%). In summary, 62.4% of the injuries occurred in the 17-21 years age group, 24.8% in the 22-25 years age group and 12.8% in the 13-16 years age group. Seventy-six percent of injuries occurred in Track athletes. Running/sprinting activities were culpable for most of the injuries (42%). Of the 134 injuries, 15.7% were low, 7.5% occurred in the muscle belly, 4.5% were high and the others were unspecified. Fifteen athletes (11.2%) had subsequent recurrences with the highest recurrence rate amongst Track & Field athletes. Only 3 of 21 low injuries and 1 of 6 high injuries recovered within 6 weeks.
Hamstring injuries are common in Jamaican athletes with a significant male preponderance. Track & Field athletes, those in the 17 to 21 years age group and those engaging in running or sprinting activities were more likely to sustain injuries. It was difficult to compare the recovery rates of high and low injuries and recurrence rates were found to closely match those in current literature.
INTRODUCTION
Hamstring injuries are not uncommon in the athletic population. In fact, they account for almost one third (29%) of all sporting injuries.1 It is the most common cause of posterior thigh pain and is quite common in recreational amateur athletes alike.2 The hamstring is actually a broad term which describes a group of three muscles in the posterior compartment of the thigh; the biceps femoris, semimembranosus and semitendinosus muscles. The proximal hamstring has a very detailed architecture and is a common site for injuries.
Injuries of the hamstring are more prevalent in sports or activities such as running or quick changes in direction that involve the stretch shortening cycle as well as in sports where there is excessive lengthening of the hamstring when the hip is in flexion.3 Acute injuries to the hamstring muscles can be one of two types. Type I hamstring strains occur during high-speed running and are more common. They usually involve the long head of the biceps femoris primarily at the musculotendinous junction.4 Track, football and rugby carry the highest incidence of type I hamstring injuries due to the sprinting demands of these sports. Type II injuries typically occur during movements involving excessive lengthening of the hamstrings with the hip in a greater degree of flexion. This injury is usually located in close proximity to the ischial tuberosity and involves the proximal free tendon of the semimembranosus. This injury is very common among dancers who employ extreme stretching techniques.5
While type I strains are associated with a more acute reduction in function, their rehabilitation period is usually shorter than type II strains. Prognosis of such an injury is commonly dependent on its location and mechanism. The rate of recurrence of these injuries lies between 12% and 31% coupled with the high probability of permanent impairment.1 This study is an epidemiological look into hamstring injuries in the Jamaican athletic population. The targeted group was athletes with hamstring injuries, who presented to the UWI Sport Medicine Clinic over a ten-year period (2007-2016). An investigation on the demographics, the type of sports or associated activity contributing to the injury, how the injury occurred, classification of the injury, length of recovery and recurrence was completed. The information from this study may be utilized to bolster prevention and rehabilitation programs in the Jamaican athletic landscape, specific sporting population and hopefully the wider Caribbean.
METHODS
A retrospective design was used to meet the objectives of the study. A census was conducted using data obtained from all of the athletes who presented to the University of the West Indies Sports Medicine Clinic with hamstring injuries during the period of interest (2007-2016). The athletes presenting to this clinic are managed by two physicians, both of whom have specialized in Sports Medicine and have more than 15 years of experience working with athletes. The approach to the clinical evaluation of hamstring injuries at the clinic is standardized and consists of observations in standing, walking and prone lying. Active movements are assessed for the lumbar spine, hip extension, standing leg swings and active knee extension in a supine position. Passive hamstring stretches are done with the patient in supine and resisted isometric testing is done for isolated knee flexion, hip extension and in combination using the single leg bridge. Palpation is done for the hamstring muscle, with focus on the musculotendinous junction and mid belly, and for the gluteal muscles. In cases where ambiguity exists, both physicians discuss the case and patients are referred for an Ultrasound or MRI. Additional tests are done to examine the lumbar spine and sacroiliac joint including the slump test which assesses neuromechanical function.
Sample size
A total of 1075 dockets were perused. One hundred and twenty-five were eligible for the study with a total of 134 hamstring pathologies.
Procedure
Ethical approval to conduct this study and the permission to collect data were granted by the Ethics Committee of the University of the West Indies and the Head of the UWI Sports Medicine Clinic respectively. The principal investigator visited the UWI Sports Medicine Clinic and reviewed the files of all the athletes who were patients there. A data extraction sheet was initially generated to collect the data and was then converted to an Excel spreadsheet.
Instruments
The principal investigator developed the instrument which looked at the demographics of the study population, the types of sports participated in, type of activity at the time of injury, method of diagnosis, anatomical details of the injured hamstring, the level of the injury and the type of hamstring pathology. Recovery and recurrence data were also obtained from the instrument.
Data Analysis
Descriptive statistics using graphs and tables were used to describe the group.
RESULTS
Demographic Data
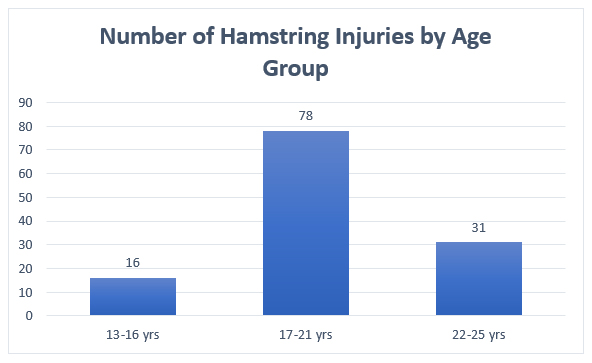
One thousand and seventy-five dockets from The UWI Sports Medicine Clinic were reviewed. 125 athletes were eligible for the study with a total of 134 hamstring injuries. Ninety-two were males (73.6%), 30 were females (24%) and data was missing for three (2.4%) athletes (all of whom had unisex names). Most of the reviewed hamstring injuries occurred in the 17-21 years age group accounting for 78 (62.4%) of the total number with 31(24.8%) injuries occurring in the 22-25 age group and 16 (12.8%) occurring in the 13-16 age group (Graph 1).
Graph 1. Bar graph showing the number of hamstring injuries by age.
Some athletes had more than one type of injury during the period of review – 8 athletes had two injuries each and one had three injuries.
Hamstring injuries by sports, level of competition and method of diagnosis
Graph 2 highlights the distribution of hamstring injuries across ten different sports: Track & Field, rugby, netball, basketball, rowing, cricket, volleyball, gymnastics, hockey and football.
Graph 2. Bar graph showing the number of hamstring injuries by sports. There were 95 Track & Field athletes with hamstring injuries which made up the majority (76%) of the studied population. Football only had 10 injured athletes (8%) while the other sports had between 0.8% and 4% of athletes with injuries. Of all the reviewed cases, 42% of injuries occurred while running, sprinting or jogging. In most of the other cases, the activity was unspecified (Graph 3).
There were 95 Track & Field athletes with hamstring injuries which made up the majority (76%) of the studied population. Football only had 10 injured athletes (8%) while the other sports had between 0.8% and 4% of athletes with injuries. Of all the reviewed cases, 42% of injuries occurred while running, sprinting or jogging. In most of the other cases, the activity was unspecified (Graph 3).
Graph 3. Bar graph showing the type of activity at the time of injury.

As it pertains to the level of competition, 61.6% of athletes were participating at the club level, 30.4% at the secondary school level and 8% were not specified. Of the 134 cases of hamstring injuries, 94.8% were diagnosed by only history and examination while 5.2% were diagnosed by history, examination and ultrasound. None of the cases required MRI for diagnosis.
Types of hamstring pathologies and anatomical classification
Strains and tears accounted for 54.2% of the total number of hamstring pathologies (Table 1).
Table 1: Summary of sports and the types of hamstring pathologies.
| Sport | Tendinitis/tendinosis/tendinopathy | Tightness | Strains/Tears |
| Cricket | 0 | 4 | 2 |
| Rugby | 1 | 0 | 1 |
| Netball | 0 | 0 | 3 |
| Gymnastics | 0 | 0 | 1 |
| Rowing | 0 | 0 | 1 |
| Basketball | 1 | 2 | 0 |
| Hockey | 0 | 3 | 2 |
| Volleyball | 1 | 0 | 0 |
| Football | 1 | 2 | 7 |
| Track & Field | 14 | 37 | 60 |
| Total | 17 | 48 | 77 |
Hamstring tightness accounted for 33.8% of the pathologies and 11.9% were categorized as tendinitis, tendinopathy or tendinosis. Track & Field athletes were affected by 78% of these pathologies. The biceps femoris was the most commonly affected muscle and accounted for 15.6% of all injuries while the semimembranosus and semitendinosus muscles accounted for 9.7% and 1.5% of the injuries respectively. Seventy-three percent of the reviewed hamstring injuries had unspecified muscles involved (Table 2).
Table 2: Summary of sports and the muscle involved.
| Sport | Muscle Injured | |||
| Biceps Femoris | Semimembranosus | Semitendinosus | Not Specified | |
| Cricket | 0 | 0 | 0 | 5 |
| Rugby | 1 | 0 | 0 | 1 |
| Netball | 1 | 0 | 0 | 2 |
| Gymnastics | 1 | 0 | 0 | 0 |
| Rowing | 0 | 0 | 0 | 1 |
| Basketball | 0 | 1 | 0 | 1 |
| Hockey | 0 | 1 | 0 | 4 |
| Volleyball | 0 | 0 | 0 | 1 |
| Football | 1 | 1 | 0 | 8 |
| Track & Field | 17 | 10 | 2 | 75 |
| Total | 21 | 13 | 2 | 98 |
Right sided hamstring injuries were marginally more common in the study population (44.5%) than left-sided injuries (38.8%) (Table3).
Table 3: Summary of sports and the anatomical location of injuries.
| Sport | Anatomical Side | |||
| Right | Left | Both | Not specified | |
| Cricket | 2 | 1 | 0 | 2 |
| Rugby | 1 | 0 | 1 | 0 |
| Netball | 2 | 1 | 0 | 0 |
| Gymnastics | 0 | 1 | 0 | 0 |
| Rowing | 1 | 1 | 0 | 0 |
| Basketball | 1 | 0 | 0 | 1 |
| Hockey | 2 | 1 | 2 | 0 |
| Volleyball | 1 | 0 | 0 | 0 |
| Football | 7 | 0 | 2 | 1 |
| Track & Field | 43 | 47 | 10 | 3 |
| Total | 60 | 52 | 15 | 7 |
Fifteen athletes (11.2%) had simultaneous injuries involving both right and left hamstrings and the anatomical side was not determined for 5.2% of study participants. Although 70.9% of the injuries were not anatomically specified, 15.9% of those that were specified were mainly low injuries. Injuries occurring in the muscle belly or mid-substance accounted for only 7.5% of the study population and high hamstring injuries accounted for 4.5%. Two athletes (1.5%) had both high and low injuries simultaneously.
Previous injuries, Recovery, Recurrence and Return to Sports
Of the 134 cases examined, 30 athletes had a previous hamstring injury at the time of diagnosis, 42 had no prior injuries and 63 were unspecified (Graph 4). The hamstring injury diagnosed for 12 of the 30 athletes with previous injuries was a recurrent injury. One was listed as a first recurrence, 5 were listed as a second recurrence and the remainder was unspecified. Of the 21 low injuries, only three fully recovered within six weeks while recovery time for the others was not specified. Of the six high injuries, only one recovered within six weeks. Fifteen athletes (11.2%) had one or more subsequent recurrent injuries – 3 athletes within less than 6 weeks (2.2%), 4 athletes between 6 weeks and 3 months (3%), 2 athletes between 4 months and 1 year (1.5%) and 6 athletes longer than 1 year (4.5%) (Table 4).
Table 4: Length of time to recurrence of hamstring injury.
| Length of time to Recurrence | Number | Percentage |
| < 6 weeks | 3 | 2.2 |
| 6 weeks- 3 months | 4 | 3 |
| 4 months- 1 year | 2 | 1.5 |
| > 1 year | 6 | 4.5 |
| Not Specified | 119 | 88.8 |
One athlete had 4 subsequent recurrences and 11 had one subsequent recurrence, the others were unspecified. As it relates to recurrence of hamstring injuries caused by sports, Track & Field had the highest number with 12 recurrences while Football had 2 recurrences and gymnastics had 1 athlete with a recurrent injury (Table 5).
Table 5: Recurrence of hamstring injuries by sport.
| Recurrence by Sports | Number | Percentage |
| Cricket | 0 | 0 |
| Rugby | 0 | 0 |
| Netball | 0 | 0 |
| Gymnastics | 1 | 0.7 |
| Rowing | 0 | 0 |
| Basketball | 0 | 0 |
| Hockey | 0 | 0 |
| Volleyball | 0 | 0 |
| Football | 2 | 1.5 |
| Track & Field | 12 | 9 |
Twenty-nine percent of athletes returned to sports while the remainder was unspecified.
DISCUSSION
This study investigated the epidemiology of hamstring injuries in the available Jamaican athletic population. It was revealed that approximately 74% of the injured athletes were male, 24% were female and 2% were unspecified. This may be since more males are involved in competitive sporting events and are more risk taking. A retrospective study that looked at gender difference in sport risk injuries and types of injuries revealed that males were at greater risk of succumbing to sporting injuries because of their significantly longer training hours.6
The majority of the hamstring injuries were found to occur in the 17-21 age group (62.4%). This can be attributed to the fact that the majority of the athletes in this age range play sports at the collegiate level. The 22-25 years age group had the second highest number (24.8%) of injuries. This finding, however, is contrary to a systematic review conducted in 2009 which stated that the risk of hamstring injuries increases with age and peaks at 23-25 years.7 The increased risk by age was attributed to “age-related muscle changes and prolonged exposure to additional risks”. Increased level of competition was also cited as a sports-specific risk for hamstring injuries.7 The finding indicating that 76% of all hamstring injuries affected Track & Field athletes is not surprising because this is one of the most popular sports in Jamaica. This corresponded with findings seen in this study’s population with club athletes being afflicted with more hamstring injuries (61.6%). It was also found that most of the injuries occurred during running activities which is in accordance with published literature.8
This research revealed that low hamstring injuries were the most common (15.7%) amongst all the injuries that were anatomically classified. Those occurring at the muscle belly were 7.5% and high injuries were only 1.5% of the total. This finding is different from that seen by Kajula et al., in which mid-substance injuries were more common compared to hamstring origin injuries.9 Type I and II hamstring injuries would have given a better idea of the anatomical location of the injury had it been used to give more precise diagnoses. This would aid in data extrapolation and comparison with existing literature. Of the muscles involved, the biceps femoris was most commonly affected and accounted for 15.6% of all recorded injuries, followed by the semimembranosus which caused 9.7% and the semitendinosus which caused 1.5% of the remaining cases. These findings closely reflect those of two studies published in 2006 and 2017 that the most common location was near the musculotendinous junction.8,10 Most of the injuries in this study were diagnosed by history and examination only. Although the majority of injuries were right-sided, the difference between right and left was not significant.
The aim of any athlete with an injury is to recover with minimal residual effects and to return to sport. In this study, the length of recovery for only 9% of the 134 injuries can be analysed because the majority of cases were unspecified. Of the 12 injuries that were documented as recovered, 7.5% recovered in less than 6 weeks while 1.5% recovered after one year. It was also revealed that 29% of athletes returned to sport. Return to sports, according to Ernlund and Vieira, is dependent on a multiplicity of factors including the type and number of muscles involved, the cross-sectional area affected and the presence of muscle edema and muscle retraction.8 For example, return to sport within days or “rapid return” could be expected with isolated lesion (<50% of the cross-sectional area) of the long head of biceps femoris. When there is musculotendinous junction involvement, lesions in multiple muscles, muscle retraction and lesions with greater than 75% cross-sectional area involvement, a delayed return which is usually greater than 2 to 3 weeks can be expected.11 There was no significant difference in the recovery rates for high and low injuries in this study.
There was an 11.2% recurrence rate among the participants in this study which closely mirrors that of previous research which examined recurrent hamstring injuries in the professional football setting.12 That study cited a recurrence rate ranging from 12%-63% and noted that the highest risk time for recurrence was the first month after return to play with elevated risk for approximately one year.12 One shortcoming of this research is that data relating to specific diagnosis of injuries, muscles involved, documentation of recovery time and recurrence of injuries and classification was minimal. Therefore, reasonable inference or extrapolations could not be drawn from the same study. It should be noted that the most accurate method of diagnosing a hamstring injury is diagnostic imaging (ultrasound or MRI) which would have only been recommended in cases where there was ambiguity in diagnosis because of its high cost. Diagnosis based on clinical evaluation can be affected by interrater reliability in performing tests. In this study, all patients seen during the period of interest were evaluated by two physicians who utilized a standardized approach that was set by the clinic. However, it is still possible that errors in diagnosis could have occurred.
CONCLUSION
Hamstring injuries are very common in the Jamaican athletic youth population. A male preponderance was demonstrated with most injuries having occurred in the 17-21 age group which is moderately contrary to existing literature. The study found that most injuries occurred in Track & Field athletes and were more likely to occur in athletes involved in running and sprinting activities. The classification of the level of injury revealed that most injuries were grouped as “not specified” which made the comparison of recovery rates between high and low injuries difficult. The rate of recurrence (11.2%) closely mirrors data presented by previous studies. Track & Field athletes suffered from the majority of recurring injuries observed within the studied population. There was no significant difference in the recovery rates for high and low injuries.
Ethical Approval: Yes
Informed Consent: Not applicable
Conflict of Interest: Nothing to declare.
Funding Statement: There is no financial affiliation, including research funding, or involvement with any of the authors or commercial organization that have a direct financial interest in any matter included in this manuscript.
Author Contributions: RBC, AM, SRM conceived and designed the study. RBC and SRM collected, analysed and interpreted the data; all authors reviewed the paper
REFERENCES
1. Ahmad, CS, Redler, LH, Ciccotti, MG, Maffulli, N, Longo, UG, Bradley, J. Evaluation and management of hamstring injuries. American Journal of Sports Medicine 2013;41(12): 2933-2947.
2. Askling, C, Schache, A. Posterior thigh pain. In: Brukner, P, Clarsen, B, Cook, J et al. Brukner and Khan’s Clinical Sports Medicine (5th ed.). Sydney, Australia: McGraw-Hill, 2016: 679-712.
3. Brooks, J, Fuller, C, Kemp, S, Reddin, D. Incidence, Risk, and Prevention of Hamstring Muscle Injuries in Professional Rugby Union. The American Journal of Sports Medicine 2006; 34: 1297-1306.
4. Brukner, P, Nealon, A, Morgan, C, Burgess, D, Dunn, A. Recurrent hamstring muscle injury: applying the limited evidence in the professional football setting with a seven-point programme. Br J Sports 2014; 48(11): 929-38.
5. Heiderscheit, BC, Sherry, MA, Silder, A, Chumanov, ES, Thelen, DG. Hamstring strain injuries: recommendations for diagnosis, rehabilitation, and injury prevention. Journal of Orthopaedics and Sports Physical Therapy 2010; 2: 67–81.
6. Ristolainen, L, Heinonen, A, Waller, B, Kujala, UM, Kettunen, JA. Gender Differences in Sport Injury Risk and Types of Injuries: A Retrospective Twelve-Month Study on Cross-Country Skiers, Swimmers, Long-Distance Runners and Soccer Players. Journal of Sports Science & Medicine 2009; 8(3): 443–451.
7. Prior, M, Guerin, M, Grimmer, K. An Evidence-Based Approach to Hamstring Strain Injury: A Systematic Review of the Literature. Sports Health 2009; 1(2): 154–164.
8. Ernlund, L, Vieira, L de A. Hamstring injuries: update article. Revista Brasileira de Ortopedia, 2017; 52(4): 373–382.
9. Kujala, UM, Orava, S, Jarvinen, M. Hamstring injuries. Current trends in treatment and prevention. Sports Med. 1997; 23: 397–404.
10. Armfield DR, Kim DH, Towers JD. Sports-related muscle injury in the lower extremity. Clin Sports Med 2006; 25: 803 – 42.
11. Askling, C, Saartok, T, Tengvar, M, Thorstensson, A. Sports related hamstring strains-two cases with different etiologies and injury sites. Scandinavian Journal of Medicine & Science in Sports 2000; 10:304–307.