
1Chandrakanth Koganti, 1Seetharaman Hariharan, 1Deryk Chen
1Anaesthesia & Intensive Care Unit, The University of the West Indies, St. Augustine, Trinidad, West Indies
Corresponding Author
Professor Seetharaman Hariharan
Professor of Anaesthesia & Critical Care medicine
Anaesthesia & Intensive Care Unit
The University of the West Indies
Eric Williams Medical Sciences Complex
Champs Fleurs, Trinidad, West Indies
E-mail: [email protected]
Copyright: This is an open-access article under the terms of the Creative Commons Attribution License which permits use, distribution, and reproduction in any medium, provided the original work is properly cited.
©2021 The Authors. Caribbean Medical Journal published by Trinidad & Tobago Medical Association.
ABSTRACT
Objectives
Dexamethasone, in the dose of 8 mg or higher, has been advocated to be used as an adjuvant to prolong the duration of brachial plexus blocks with local anaesthetics. This study aimed to test the hypothesis that a lower dose of dexamethasone (4 mg) added to bupivacaine would prolong the duration of analgesia in brachial plexus blocks.
Methods
A randomized double-blind placebo-controlled trial was conducted on patients who underwent supraclavicular brachial plexus blocks using an ultrasound. Patients were randomized to receive 19 mL of 0.5% bupivacaine with dexamethasone (4 mg) (study group) and saline (1 mL) (control group). Primary outcome measure was the duration of analgesia. Onset and duration of sensory, motor blocks, postoperative 24-hour morphine requirements were also recorded.
Results
A total of 46 patients were studied with 24 patients in the dexamethasone group and 22 patients in the control group. Demographic data, type and duration of surgery were comparable between the groups. Dexamethasone group patients had significantly longer duration of analgesia [Mean (SD): 19.8 (3.8) hours], compared to control group patients [Mean (SD): 14.5 (4.2); p< 0.001]. Morphine requirements over a 24-hour period were not significantly different between the groups.
Conclusion
Low-dose dexamethasone significantly prolongs the duration of analgesia when used with bupivacaine in supraclavicular brachial plexus blocks, although it does not significantly decrease the overall opioid requirements for 24 hours postoperatively.
Keywords: brachial plexus blocks, dexamethasone, adjuvant, analgesia
INTRODUCTION
Adequate postoperative pain control is an important component of care of the surgical patient and inadequate pain management may lead to many undesirable effects including patient discomfort, prolonged recovery, prolonged hospital-stay and chronic pain.1 Opioids continue to be the mainstay of therapy for postoperative pain. Patient-controlled analgesia (PCA) with opioids is one of the effective methods to control postoperative pain, although the side effect profile of the opioids such as nausea, vomiting, respiratory depression, bradycardia, pruritus are some concerns. In addition, the use of PCA with opioid infusions in the postoperative surgical wards is often constrained by poor monitoring, lack of adequately trained nursing staff, equipment failure, etc., which is especially true in settings like ours. Lack of consistent operation of acute pain services may also be attributable for suboptimal management of pain in our setting.
Peripheral nerve blockade has been in use since 1911 and is one of the promising modalities for intraoperative and postoperative analgesia. Published studies show better perioperative outcomes in patients receiving peripheral nerve blocks compared to those receiving intravenous opioids in orthopaedic surgery.2 The advantages included shorter hospital stays, improved joint range of motion, low pain scores, and lower opioid requirements.2
Brachial plexus block provides adequate anaesthesia and analgesia for upper limb surgeries and can be solely used without the need for general anaesthesia. The supraclavicular approach is commonly used for surgery of the arm, below the shoulder joint. The plexus is superficial and compact and can be easily blocked using a relatively smaller amount of local anaesthetic solution. Traditionally, the block has been performed by blind paraesthesia methods or with the help of a peripheral nerve stimulator; nowadays, ultrasound is being increasingly used to assist performing this block, which not only increases the safety but also decreases the total amount of local anaesthetics used.
The duration of analgesia after a single-shot supraclavicular block depends on the type of local anaesthetic used.3-5 Although single-shot nerve blocks may provide good intraoperative and early postoperative analgesia, the overall duration of analgesia is short-lived and may pose a problem for patients discharged on the same day. One of the suggested modalities to extend the duration of block is the use of perineural catheters, which do provide sufficient pain relief but may not be very cost-effective.6 Indwelling catheters for peripheral nerve blocks also carry the risk of infection and migration. Due to the lack of equipment and limited resources, catheter techniques are not being used in our setting.
Adjuvants such as adrenaline, clonidine, dexamethasone, midazolam, fentanyl, and neostigmine have been used in many studies to prolong the duration of peripheral nerve blocks.7-10 Ideally, the adjuvants should not only prolong the duration of analgesia, but also should have minimal side effects and be cost-effective.
Dexamethasone is one of the easily available drugs with minimal side effects, if used in the least possible dose. Previous studies have demonstrated the effectiveness of a higher dose (8 mg) of dexamethasone as an adjuvant in the brachial plexus blocks.3-5 11 A relatively recent study used low-dose dexamethasone, but 25 mL of levobupivacaine for the brachial plexus blocks.12
With this background, the present study was designed to evaluate the effect of low-dose dexamethasone on the duration of analgesia in brachial plexus block with bupivacaine. This study is different not only in that the dose of dexamethasone is lower, but also the volume and dose of local anaesthetics also are decreased when compared to the published research.
METHODS
After approval from the Ethics Committee of the University of the West Indies, patients undergoing upper limb surgeries were enrolled in the study. Written informed consent was obtained. The study was designed as a prospective double blind randomized controlled study. Patients were randomly assigned to one of the following two groups by computer allocation:
Group I (Control):
Patients in this group received 19 mL of 0.5% bupivacaine and 1 mL of saline.
Group II (Study):
Patients in this group received 19 mL of 0.5% bupivacaine and 1 mL (4 mg) of dexamethasone.
Inclusion criteria
- Age 18–80 years
- American Society of Anaesthesiologists I & II patients of any gender
- Upper limb surgery below the shoulder joint (both elective & emergency surgery)
Exclusion criteria
- Patient refusal
- Contraindication for the block which include neurological deficit involving brachial plexus, respiratory insufficiency, when bilateral block is necessary
- Pregnant women
- Peptic ulcer disease
- Allergy to local anaesthetics
- Long term steroid therapy
- Any bleeding disorder
- Local infection at the injection site
Procedure
Patients were randomized to one of the two groups using a computer and the group assignment was sealed in an envelope. The anaesthesiologist involved in the performance of the block was blinded to the group allocation.
Intravenous fluid was started and standard monitoring was done with blood pressure, SpO2 and ECG. Ultrasound guidance with a linear high-frequency probe was used to localize the brachial plexus by the supraclavicular approach. Scanning was done in the supraclavicular area for identification of the subclavian artery, first rib, brachial plexus and pleura. Brachial plexus was identified as a cluster of hypoechoic nodules. After cleaning the supraclavicular area with DuraPrep™, 3 mL of 2% lidocaine was used for skin infiltration 1–2 cm lateral to the probe. Patient was positioned 30-45° head up and a sand bag was placed under the ipsilateral shoulder to facilitate the performance of the block. 22-gauge 2-inch Stimuplex™ stimulator needle was used along with a peripheral nerve stimulator as an additional tool to detect proximity to the nerves, although intraneural injection was not specifically assessed. The block solution was first injected at the “corner pocket” of the subclavian artery and first rib to block the inferior trunk of the brachial plexus. The second injection was done more superficially to block the superior trunk of the brachial plexus. Repeated aspirations were done before injection to prevent inadvertent intravascular administration. After injection of the local anaesthetic, the patient was assessed for sensation to pinprick every 2 minutes until there was loss of sensation in the musculocutaneous, median, radial and ulnar nerve distribution. The time from injection of local anaesthetic to obliteration of sensation to pinprick was considered as the onset of sensory block. The extent of motor blockade was tested in the distribution of radial (thumb abduction), ulnar (thumb adduction), median (thumb opposition), musculocutaneous (flexion at the elbow) and evaluated using a 3-point scale where 2 = normal movement, 1 = paresis, 0 = no movement. Onset of motor block was assessed from the time of injection, to decrease in strength (paresis). Duration of surgery, tourniquet time, and intraoperative opioids usage were noted. Intraoperative opioids (fentanyl 0.5–1 μg/kg) were given to patients as a supplemental analgesic to all patients. No additional general anaesthesia was given.
Postoperatively, during the recovery period, the patient was assessed for pain using the Visual Analog Pain Score in the scale of 0–10; 0 being ‘no pain’ and 10 being ‘worst pain’. Any pain score above 3 was treated with morphine in 2–4 mg increments until the patient was comfortable. Blood glucose was checked in the recovery room 30 minutes after surgery before discharging to the ward. Postoperatively, the patient was assessed at 4 hours and 16 hours after discharge from the recovery room. Total consumption of opioids, paracetamol, and ibuprofen in the first 24 hours was noted. Contact numbers of all the patients were taken. Patients who were discharged before the 24 hours were contacted to find about the block, although these patients did not receive any prescription for oral opioids. All patients were followed up by the anaesthesiologist who was blinded to the group allocation of the patient. All opioids consumed were converted to morphine equivalents.
Primary outcomes:
- Duration of analgesia: Time interval from the end of injection of local anaesthetic to the first appearance of pain at the surgical site or first request to rescue analgesia.
Secondary outcomes:
- Duration of motor block: Time interval from the end of injection of local anaesthetic to return of motor power
- Onset of sensory block
- Onset of motor block
- VAS score in the recovery, 4 hours after discharge, 16 hours after discharge
- PACU blood glucose
- 24-hour opioid requirements
The sample size calculation took into account the probability of the study detecting a treatment difference at a two-sided 0.05 significance level to be 91%. The calculated sample size for the present study was 46 patients (23 in each group).
Other than the comparisons between study and control groups, analyses were also done to determine if there were differences in duration of analgesia in different types of surgical cases categorizing patients into groups based on less and severe pain intensity. Cases such as tendon repair, K-wiring and arteriovenous (AV) fistula placement were considered to have less pain intensity and classified under the ‘mild pain’ category. Cases such as open reduction and internal fixation of the humerus, or radius and ulna were considered to have moderate to severe pain intensity and were classified under the ‘severe pain’ category.
Statistical analysis was done using Statistical Package for Social Sciences (SPSS) – Version 13 software package. Descriptive analysis was done for demographic data such as age, gender, ethnicity, weight, height, BMI and type of procedure. Data were analysed using independent ‘t’ test; p value < 0.05 was fixed to be statistically significant.
RESULTS
A total of 53 patients were selected and enrolled in the study after fulfilling the eligibility criteria and signing the consent form. Enrolment started in August 2013; data collection was completed by March 2014. Out of the 53 patients, 3 had failed blocks and 4 patients were lost to follow up. The flow chart below shows the enrolment of the patients and randomization to saline and dexamethasone group. A total of 46 patients were finally analysed for the primary and secondary outcomes.
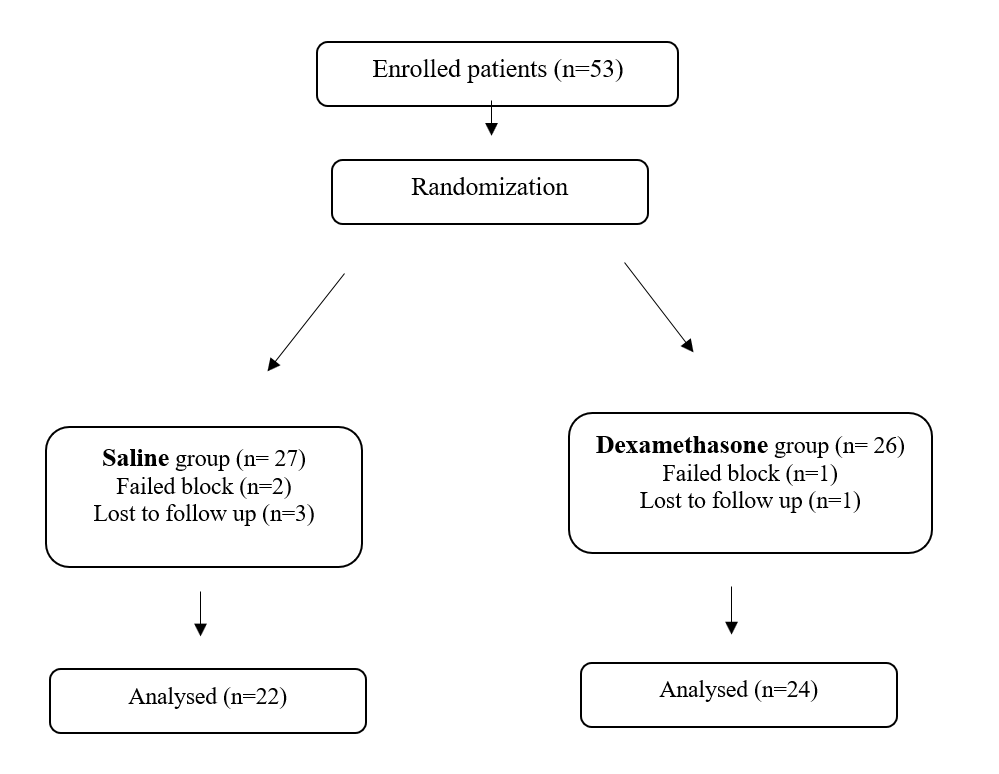
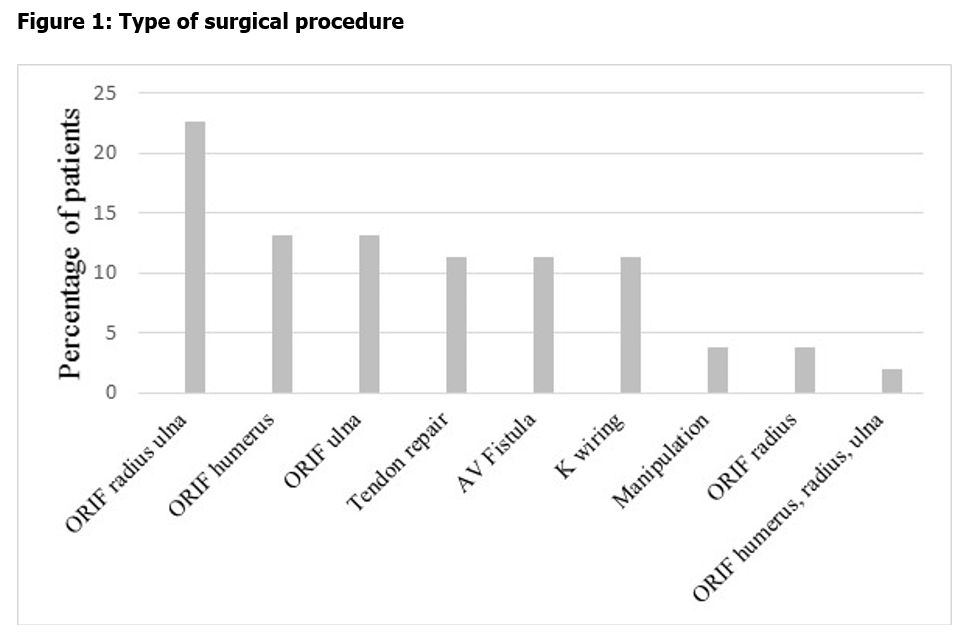
Figure 1: Type of surgical procedure
The overall age of the patients ranged from 17–80 years (median 33 years). The ages of the patients in both the groups were comparable. Mean age in the saline group was 42.6 years (SD 15.8), and in the dexamethasone group, the mean age was 37.1 years (SD 16.4). Among the 46 patients, 13 were female and 33 were male. Overall, 35 patients belonged to ASA I Grade physical status, 4 patients were ASA II and 7 belonged to ASA III.
The body weight of the patients ranged from 50 to 136 kg; [mean 74.7 (SD 16.9)]. Height of the patients ranged from 152.5–188 cm; [mean 172.5 cm (SD 7.4)]. The body mass index (BMI) of the patients ranged from 17.3–44.5; [mean 25.3 (SD 5.4)]. The BMI of the patients in each group were comparable. Mean BMI in the saline group was 24.5 (SD 3.8), and was 26.6 (SD 6.4) in the dexamethasone group.
The site of surgical procedure included upper arm, elbow, forearm and hand. Among the different sites, surgeries for forearm and below comprised 73.6% of all procedures; upper arm surgeries were 13.2%, whereas elbow surgeries were 7.5%. One patient had both upper arm and forearm surgery as a combined procedure.
Figure 1 shows the distribution of the different orthopaedic procedures done. Overall, open reduction and internal fixation (ORIF) of radius and ulna comprised around 22.6% of the total procedures done.
Surgical duration between the two groups was comparable. Mean duration of surgery in saline group was 102.3 minutes (SD 63.8). Mean duration of surgery in dexamethasone group was 98 minutes (SD 60.6). Table 1 shows the comparison of different variables including BMI, surgery duration, post-anaesthesia care unit (PACU) random blood sugar and tourniquet time between the groups.
Table 1: Comparison between groups
| Variable | Saline
Mean (SE) (n=22) |
Dexamethasone
Mean (SE) (n=24) |
P value* |
| Age (y) | 42.6 (3.3) | 37.1(3.3) | 0.251 |
| Surgery duration (min) | 102.3 (13.3) | 98 (12.3) | 0.815 |
| Onset sensory (min) | 9.1 (2) | 7 (0.9) | 0.35 |
| Onset motor (min) | 12.9 (2.7) | 8.6 (1.7) | 0.19 |
| Intraoperative morphine equivalents (mg) | 5.2 (1.3) | 1.7 (0.7) | 0.023 |
| PACU morphine equivalents (mg) | 0.4 (0.3) | 1.3 (0.5) | 0.202 |
| PACU blood sugar (mg/dL) | 82.8 (15.2) | 83.8 (10.4) | 0.95 |
| Sensory block duration (min) | 875.2 (54.9) | 1190.7 (47.4) | <0.001 |
| Motor block duration (min) | 833.9 (62.2) | 1058.7 (64.8) | 0.016 |
| 24-hour morphine equivalents (mg) | 4.5 (1.7) | 3.2 (1.2) | 0.551 |
* p-value by independent t-test
There was no significant difference in the onset times for sensory or motor blockade. Mean duration of analgesia in the saline group was 875.2 minutes. Mean duration of analgesia in dexamethasone group was 1190.7 minutes. Duration of analgesia was significantly prolonged in dexamethasone group when compared to saline group (p < 0.001). The duration of motor block was also prolonged in dexamethasone group (p= 0.02).
All analgesic requirements were quantified by calculating morphine equivalents for the analgesics used in all patients. Overall, for all patients, intraoperative analgesic requirement was less in the dexamethasone group when compared to the saline group (p=0.02). There was no significant difference in PACU analgesic requirements between the groups. PACU random blood sugar was comparable between two groups (p=0.96). In addition, 24-hour opioid requirements also did not differ between the two groups (p= 0.55).
According to the pain intensity, there were 21 patients in the ‘mild pain’ category, of which 11 patients received bupivacaine and saline, and 10 cases received bupivacaine and dexamethasone. In the ‘moderate to severe’ group, there were 25 cases of which 11 cases received saline and 14 cases received dexamethasone. The comparisons between these groups are shown in Table 2. In both categories, the sensory block was significantly different and there was no difference in the motor blockade.
Table 2: Comparison of groups in surgeries according to pain intensity
| Saline
Mean (SE) |
Dexamethasone
Mean (SE) |
P value* | |
| Mild pain intensity group | |||
| Sensory block duration | 898 ± 88.4 | 1232.4 ± 63.5 | 0.009 |
| Motor block duration | 887 ± 87.1 | 1095.7 ± 87.2 | 0.1 |
| Moderate to severe pain intensity group | |||
| Sensory block duration | 829 ± 71.5 | 1190 ± 66.3 | 0.001 |
| Motor block duration | 770 ± 96.8 | 1004.4 ± 91.5 | 0.09 |
*p-value by independent t-test
DISCUSSION
The results of our study demonstrate that the addition of even a low dose (4 mg) dexamethasone to bupivacaine prolonged the duration of analgesia after supraclavicular brachial plexus block when compared to a control group receiving saline. The findings of the study are comparable to earlier reports, where dexamethasone was used in higher doses.13-15 In addition, the volume of bupivacaine used in our study was also less when compared to those reports.
The onset of sensory and motor block did not differ between the groups which was similar to that observed by other authors in their study using mepivacaine.3 An earlier study reported an early onset of sensory block in the dexamethasone group.16 This might have been due to the use of lidocaine with adrenaline along with bupivacaine, and also the large volume (40–50 mL) of local anaesthetic used.
In a retrospective study of 1040 patients, who had upper and lower extremity peripheral nerve blocks, authors found that dexamethasone when added to 0.5% ropivacaine increased the median block duration by 37% in both limbs.17 Although both 8 mg and 4 mg doses of dexamethasone were used, the effect was reported as same with both the doses.
The mean duration of motor block in our study was longer than the duration observed by Shaikh et al (846 min).14 The duration was shorter than that observed by Tandoc et al (2202 min).18
In our study, the intraoperative opioid use was significantly lower in the dexamethasone group compared to control group, although there was no difference in the amount of opioid used in the PACU. The possible reason for this finding may be that comparatively more intraoperative opioids were used in control group patients, and its effect might have lasted into the recovery period.
A previous meta-analysis regarding the use of perioperative intravenous dexamethasone showed a small but significant elevation of blood sugar at 24 hours after the operation.19 An earlier study compared intravenous and perineural administration of 10 mg dexamethasone in patients who had shoulder surgery under interscalene block using ropivacaine.20 Although the duration of analgesia was similar irrespective of the route of administration, there was an increase in mean postoperative blood glucose in groups receiving dexamethasone. In the present study, there was no significant increase in the blood sugar levels. The possible reasons may be the lower dose of dexamethasone, as well as the administration of dexamethasone perineurally. Systemic effects of perineurally administered dexamethasone are not clearly known. The effect of perineural dexamethasone on blood sugar levels have not been well studied, but it has been shown to decrease the incidence of postoperative nausea and vomiting.3
Dose-dependent effect of dexamethasone has been described in a previous study in gynaecological surgery patients.21 This study reported less opioid consumption in patients receiving a higher dose of dexamethasone (0.1 mg/kg) compared to those receiving a lower dose (0.05 mg /kg).
There also has been a recent trial in 39 patients comparing perineural and intravenous administration of low-dose dexamethasone for prolonging the duration of interscalene block with ropivacaine. This trial concluded that perineural, but not intravenous dexamethasone, prolonged the duration of analgesia.22
In the present study, the total opioid consumption in the first 24 hours after surgery did not differ significantly between the groups, which was similar to a previous study, which quantified 72 hours opioid consumption.4 In addition, the VAS pain scores at recovery, at 4 hours and at 16 hours were not different between the two groups in the present study. This is in contrast to the study done by Cummings et al where VAS scores were low in the dexamethasone group on postoperative day 1 and higher on postoperative day 3 compared to the saline group.4
The mechanism of action of dexamethasone via the perineural route is still not fully understood. Some of the proposed mechanisms include suppression of transmission in unmyelinated C-fibres and upregulation of K channels.23 24 The ectopic neuronal discharge from an experimental neuroma is prevented by application of corticosteroid, suggesting a direct membrane effect of the corticosteroid.25 Safety of perineural use of dexamethasone has also been studied. A previous study found that even high concentrations of adjuvants like dexamethasone in combination with clonidine, buprenorphine, midazolam were significantly less neurotoxic when compared to ropivacaine.26 Two meta-analyses on the use of dexamethasone found no increase in the incidence of infection or delayed wound healing or any major adverse effects.19 27 Perineal pruritus has been described after an intravenous bolus administration of dexamethasone.28 None of the patients in our study experienced any side effects.
The study had some limitations. All cases of upper limb surgery below the shoulder joint were included in this study. This included different type of surgeries with different level of expected pain intensity. The durations of the surgery were also different, although it was comparable among the groups. It may be possible that this difference in type of surgery had influence in pain scores and duration of block. In reported similar studies done previously, all the patients had the same surgery, often performed by the same surgeon.
Nevertheless, in conclusion, the addition of 4 mg dexamethasone to bupivacaine prolongs the postoperative analgesia after supraclavicular block for patients undergoing surgery of the upper limb below the shoulder joint. Intraoperative opioid requirements were low when dexamethasone was used. However, the overall postoperative opioid requirements and VAS pain scores were not significantly different with the use of dexamethasone as an adjuvant. PACU blood glucose readings were also unaffected by the use of dexamethasone in the dose of 4 mg.
Ethical Approval statement: This study was approved by the ethics committees of the University of the West Indies, St Augustine.
Conflict of interest statement: None
Informed Consent statement: Not Applicable
Funding statement: None
Authors Contribution: Seetharaman Hariharan conceptualised and supervised the research, analysed the data and wrote the manuscript. Chandrakanth Koganti conducted the research, collected data and contributed in writing the manuscript. Deryk Chen contributed in the research methodology. All three authors critically reviewed the manuscript and approved its final version for submission.
REFERENCES
- Hariharan S, Chen D, Morapedi O, Bathusi D, Segakolodi B, Sejeso K. Prescribing patterns of analgesics and pain relief in hospitalized trauma patients in a tertiary care teaching hospital of a Caribbean developing country. Journal of Pain Management 2010; 3 (3): 241-246
- Hebl JR, Dilger JA, Byer DE, Kopp SL, Stevens SR, Pagnano MW, Hanssen AD, Horlocker TT. A pre-emptive multimodal pathway featuring peripheral nerve block improves perioperative outcomes after major orthopedic surgery. Reg Anesth Pain Med. 2008 Nov-Dec; 33(6):510-7.
- Parrington SJ, O’Donnell D, Chan VWS, et al. Dexamethasone added to mepivacaine prolongs the duration of analgesia after supraclavicular brachial plexus blockade. Reg Anesth Pain Med 2010; 35: 422–426.
- Cummings KC, Napierkowski DE, Parra-Sanchez I, et al. Effect of dexamethasone on the duration of interscalene blocks with ropivacaine or bupivacaine. Br J Anaesth 2011; 107 (3): 446–453
- Pathak RG, Satkar AP, Khade RN. Supraclavicular brachial plexus block with and without dexamethasone – A Comparative Study. International Journal of Scientific and Research Publications. 2012; 2(12):1–7.
- Joshi G, Gandhi K, Shah N, Gadsden J, Corman SL. Peripheral nerve blocks in the management of postoperative pain: challenges and opportunities. J Clin Anesth. 2016 Dec; 35:524-529. doi: 10.1016/j.jclinane.2016.08.041.
- Van Elstraete AC, Pastureau F, Lebrun T, Mehdaoui H. Neostigmine added to lidocaine axillary plexus block for postoperative analgesia. Eur J Anaesthesiol. 2001 Apr; 18(4):257-60.
- Moharari R, Sadeghi J, Khajavi M, Davari M, Mojtahedzadeh M. Fentanyl supplement expedites the onset time of sensory and motor blocking in interscalene lidocaine anesthesia. Daru. 2010; 18(4):298-302.
- Shaikh SI, Veena K. Midazolam as an adjuvant in supraclavicular brachial plexus block. Anaesth Pain & Intensive care. 2012; 16 (1):7-11.
- Agarwal S, Aggarwal R, Gupta P. Dexmedetomidine prolongs the effect of bupivacaine in supraclavicular brachial plexus block. J Anaesthesiol Clin Pharmacol. 2014 Jan-Mar; 30(1): 36–40.
- Baloda R, Bhupal JPS, Kumar P, Gandhi GS. Supraclavicular Brachial Plexus Block with or without Dexamethasone as an Adjuvant to 0.5% Levobupivacaine: A Comparative Study J Clin Diagn Res. 2016 Jun; 10(6): UC09–UC12. doi: 10.7860/JCDR/ 2016/18325.8048
- Persec J, Persec Z, Kopljar M, Zupcic M, Sakic L, Zrinjscak IK, Marinic DK. Low-dose dexamethasone with levobupivacaine improves analgesia after supraclavicular brachial plexus blockade. Int Orthop. 2014 Jan; 38(1):101-5.
- Shrestha BR, Maharjan SK, Shrestha S, Gautam B, Thapa C, Thapa PB, Joshi MR. Comparative study between tramadol and dexamethasone as an admixture to bupivacaine in supraclavicular brachial plexus block. JNMA J Nepal Med Assoc. 2007 Oct-Dec; 46(168):158-64.
- Shaikh MR, Majumdar S, Das A, Saha TK, Bandyopadhyay SN, Mukherjee D, Mahawar S. Role of Dexamethasone In Supraclavicular Brachial Plexus Block. IOSR-JDMS. 2013 Nov-Dec; 12(1):01-07.
- Vieira PA, Pulai I, Tsao GC, Manikantan P, Keller B, Connelly NR. Dexamethasone with bupivacaine increases duration of analgesia in ultrasound-guided interscalene brachial plexus blockade. Eur J Anaesthesiol. 2010 Mar; 27(3):285-8.
- Shrestha BR, Maharjan SK, Tabedar S. Supraclavicular brachial plexus block with and without dexamethasone – a comparative study. Kathmandu Univ Med J (KUMJ). 2003 Jul-Sep; 1(3):158-60.
- Rasmussen SB, Saied NN, Bowens C Jr, Mercaldo ND, Schildcrout JS, Malchow RJ. Duration of Upper and Lower Extremity Peripheral Nerve Blockade Is Prolonged with Dexamethasone When Added to Ropivacaine: A Retrospective Database Analysis. Pain Med. 2013 Aug; 14 (8): 1239–1247.
- Tandoc MN, Fan L, Kolesnikov S, Kruglov A, Nader ND. Adjuvant dexamethasone with bupivacaine prolongs the duration of interscalene block: a prospective randomized trial. J Anesth. 2011; 25(5):704-709.
- Waldron NH, Jones CA, Gan TJ, Allen TK, Habib AS. Impact of perioperative dexamethasone on postoperative analgesia and side-effects: systematic review and meta-analysis. Br J Anaesth 2013; 110 (2): 191–200
- Desmet M, Braems H, Reynvoet M, Plasschaert S, Van Cauwelaert J, Pottel H, Carlier S, Missant C, Van de Velde M. I.V. and perineural dexamethasone are equivalent in increasing the analgesic duration of a single-shot interscalene block with ropivacaine for shoulder surgery: a prospective, randomized, placebo-controlled study. Br J Anaesth. 2013 Sep; 111(3):445-52.
- De Oliveira GS Jr, Ahmad S, Fitzgerald PC, Marcus RJ, Altman CS, Panjwani AS, McCarthy RJ. Dose ranging study on the effect of preoperative dexamethasone on postoperative quality of recovery and opioid consumption after ambulatory gynaecological surgery. Br J Anaesth. 2011 Sep; 107(3):362-71.
- Kawanishi R, Yamamoto K, Tobetto Y, Nomura K, Kato M, Go R, Tsutsumi YM, Tanaka K, Takeda Y. Perineural but not systemic low-dose dexamethasone prolongs the duration of interscalene block with ropivacaine: a prospective randomized trial. Local Reg Anesth. 2014 Apr 5; 7:5-9.
- Johansson A, Hao J, Sjölund B. Local corticosteroid application blocks transmission in normal nociceptive C-fibres. Acta Anaesthesiol Scand. 1990 Jul; 34(5):335-8.
- Attardi B, Takimoto K, Gealy R, Severns C, Levitan ES. Glucocorticoid induced up-regulation of a pituitary K+ channel mRNA in vitro and in vivo Receptors Channels. 1993; 1(4):287-93.
- Devor M, Govrin-Lippmann R, Raber P. Corticosteroids suppress ectopic neural discharge originating in experimental neuromas. Pain. 1985 Jun; 22(2):127-37.)
- Williams BA, Hough KA, Tsui BY, Ibinson JW, Gold MS, Gebhart GF. Neurotoxicity of adjuvants used in perineural anesthesia and analgesia in comparison with ropivacaine. Reg Anesth Pain Med. 2011 May-Jun; 36(3):225-30
- Choi S, Rodseth R, McCartney CJ. Effects of dexamethasone as a local anaesthetic adjuvant for brachial plexus block: a systematic review and meta-analysis of randomized trials. Br J Anaesth. 2014 Mar; 112(3):427-39.
- Perron G, Dolbec P, Germain J, Béchard P. Perineal pruritus after IV dexamethasone administration. Can J Anaesth. 2003 Aug-Sep; 50(7):749-50.